Introduction
Naval medical treatment facilities (MTFs) can adopt certain technologies to aid in reducing preanalytical errors. These errors threaten the quality of patient care by deferring its delivery or creating costly inefficiencies. The preanalytical process entails all procedures beginning from sample collection to when the sample can be analyzed by a processing laboratory (Lippi et al., 2013). Unsurprisingly, the bulk of preanalytical errors occur outside of the receiving laboratory and nearer to the point of collection, such as within clinics or inpatient wards. They may include mislabeled samples, inappropriate collection procedures, or samples sent to a processing laboratory without requisite physician orders. Though the causes of preanalytical errors are numerous, the consequent result is monolithic; that is, the cost of health care delivery increases while health care quality diminishes.
In the face of such “man-made” challenges, the Naval Medical Center San Diego (NMCSD) is no more immune than the dozens of MTFs that dot the contiguous landscape. Indeed, as the medical hub of the western seaboard, receiving over 1.2 million outpatient visits in 2014 alone, NMCSD has few equals within the cohort of MTFs (Naval Medical Center San Diego, 2016). Accordingly, process and technological improvements are incumbent to its mission of providing optimized care to the military community. To this end, I will review how the use of barcode scanning technology can reduce the number of preanalytical errors stemming from a failure to input provider orders before a specimen is transported.
The process of sample collection and transport at NMCSD differs little from other military MTFs. To begin, a patient is checked-in by medical personnel and subsequently transported to a treatment area (Figure 1). There, assessment occurs, and verbal orders may be given to inform sample collection procedures. Following this, barcode labels containing patient identifiers are generated and affixed to the samples, before being transported to the laboratory for processing.
At various points in this process, preanalytical errors can occur. To begin with, if verbal (not written) orders are given, which often occurs during emergencies, inappropriate samples might be collected as a result of the misunderstandings and assumptions that arise (Lippi et al., 2013). In addition, barcode-generated labels may be affixed to the wrong sample, or samples transported to the laboratory before orders are input in the laboratory information system (LIS). Tracking these infractions can be challenging for any MTF, especially one as large and heavily trafficked as NMCSD. Thus, in light of such challenges, effective uses of technology and robust quality assurance programs are instrumental in optimizing sample processing procedures, while also controlling errors (Lillo et al., 2012). These programs may entail suggesting process improvement, organizing interdepartmental consortiums that focus on emerging challenges, or identifying reasons for trends or recurrences. Moreover, proper training in medical procedures and competencies in the use of available technology is also integral to optimizing healthcare delivery.
Concerning sample processing nearer to the point of collection, the use of barcode scanners that are interfaced with LIS can dramatically reduce the number of preanalytical errors (Pantanowitz & Parwani, 2014). To understand how, consider the following not uncommon scenario first involving samples that originated from the NMCSD Emergency Department (ED), or to a lesser extent, the satellite inpatient wards. Following a patient assessment, lab orders may be given verbally thus allowing sample collection to occur sooner. However, orders not subsequently input in LIS, in advance of specimens transport to the processing laboratory, are not readily identified nearer to the point of collection (Figure 1). Thus, the processing laboratory receives labeled barcoded samples but is unable to accession them for specimen processing, in the absence of provider orders. Consequently, patient care is delayed, and sample stability is adversely impacted, especially for more sensitive laboratory assays. In response to these types of scenarios, which occur dozens of times daily, the processing laboratory will telephone the ED or the ward where patient assessment occurred. Exasperating the situation, samples often arrive continuously and may even overwhelm pneumatic tube stations (Lillo et al., 2012). This aggregates efforts to determine the requesting location. Further, the processing technician may be different from the one who delivered the samples from each pneumatic station, thereby, complicating discernment further. Finally, efforts to locate the patient using LIS are not always fruitful due to information not being readily updated, especially when patients are transferred between wards (Snyder et al., 2012). Hence, laboratory technicians become tasked with “figuring out” the patient’s requesting location so that the provider or notifying the attending nurse to input orders in LIS. Meanwhile, the collected samples remain unprocessed until the orders are entered.
Such inefficiencies and preanalytical errors can be eliminated if the requesting location verifies orders before specimen transport. However, computer terminals and pneumatic tube system stations are not always nearby. Further, the requirement of CAC-enabled login at military MTF to access internal systems further restricts the terminals that medical personnel can access, and thus prohibits efficient verification (Snyder et al., 2012). Thus, it becomes easier to assume that the appropriate orders are reflected in LIS instead of verifying if this is indeed the case. This predicament is further amplified by the fact that the medical personnel collecting the sample may be different from the provider requesting the labs, who may also differ from the person delivering the samples to the pneumatic tube system.
Installing barcode scanning devices in terminals interfaced with LIS and in proximity to pneumatic tube system stations can potentially eliminate these scenarios from occurring, and by extension, the preanalytical errors they generate (Lippi et al., 2013). Thus, efficient verification can happen closer to the point of collection, which will reduce the number of samples transported to the laboratory without inputted provider orders. Moreover, discrepancies stemming from the wrong sample type collected (e.g., plasma samples for tests that require serum) can quickly be identified using the LIS interface just before its transportation to the processing laboratory (Snyder et al., 2012). Scanning the barcode of each sample using the affixed label, and reviewing patient identifiers, the lab tests ordered, and specimen requirements can be conveniently visualized by users, resulting in corrective actions being initiated sooner by those more directly involved in the care of the patient.
As an example, consider the previous scenario involving the Emergency Department samples. If barcode scanning terminals interfaced with LIS were installed near pneumatic tube stations, the discovery of samples without provider orders would occur within the ED (closer to the point of collection) (Figure 2). At this stage, the medical personnel would locate the attending nurse or physician and request that orders be input – unless of course the person doing the verification is the attending nurse or physician (Snyder et al., 2012). Thus, the laboratory upon receipt of the specimens can begin processing without delay, negating the need to contact the requesting location for reasons involving missing orders, incorrect sample submitted, and so forth.
The use of barcode scanning technology is already ubiquitous within the American society including in grocery store, pharmacy, and hospital settings. Moreover, the technology is also utilized by the NMCSD Main Laboratory to scan samples delivered through the pneumatic tube system. Thus, adapting this technology for use within the various requesting locations that regularly transport samples to the laboratory would reduce the number of preanalytical errors that occur in military MTFs including NMCSD. Moreover, the related costs of purchasing, installing, and maintaining the technology can likely be recovered in the form of decreases in the length of hospitalization, increases in laboratory productivity, and other improvements in the optimization of health care delivery (Snyder et al., 2012).
NMCSD and other military MTFs stand to benefit from adopting LIS-interfaced, barcode scanning technology. By installing LIS supported terminals outfitted with barcode scanning technology in proximity to pneumatic tube stations, can streamline sample verification and reduce preanalytical errors. Thus, the consequent processing delays and inefficiencies that such errors create would be reduced if not eliminated. Vigorous review and improvement of existing processes, and, to that end, leveraging the proven technology, is paramount to both the efforts of naval medicine and the Department of Defense at large, in providing the greatest quality of care to members of the uniformed services and their dependents. Thus, we owe it to ourselves and the communities to which we serve, to eliminate the opportunities for errors such as these to occur. Hence, by adopting these process improvements through LIS-interfaced barcode scanning terminals, we honor not just ourselves but those whose health we are charged with protecting.
References
Chan, J. C. W., Chu, R. W., Young, B. W. Y., Chan, F., Chow, C. C., Pang, W. C., … & Leung, P. M. (2004). Use of an electronic barcode system for patient identification during blood transfusion: 3-year experience in a regional hospital. Hong Kong Medical Journal, 10(3), 166-171.
Lillo, R., Salinas, M., López Garrigós, M., Naranjo Santana, Y., Gutiérrez, M., Marín, M. D., … & Uris Sellés, J. (2012). Reducing preanalytical laboratory sample errors through educational and technological interventions.
Lippi, G., Becan-McBride, K., Behúlová, D., Bowen, R. A., Church, S., Delanghe, J., … & Nikolac, N. (2013). Preanalytical quality improvement: in quality we trust. Clinical Chemistry and Laboratory Medicine, 51(1), 229-241.
Naval Medical Center San Diego, (2016). Why NMC San Diego? Med.navy.mil. Retrieved 22 March 2016, from http://www.med.navy.mil/sites/nmcsd/pages/visitors/why.aspx
Pantanowitz, L., & Parwani, A. (2014). Practical Informatics for Cytopathology. Springer Science & Business Media.
Snyder, S. R., Favoretto, A. M., Derzon, J. H., Christenson, R. H., Kahn, S. E., Shaw, C. S., … & Tanasijevic, M. J. (2012). Effectiveness of barcoding for reducing patient specimen and laboratory testing identification errors: a Laboratory Medicine Best Practices systematic review and meta-analysis. Clinical Biochemistry, 45(13), 988-998.
Appendix
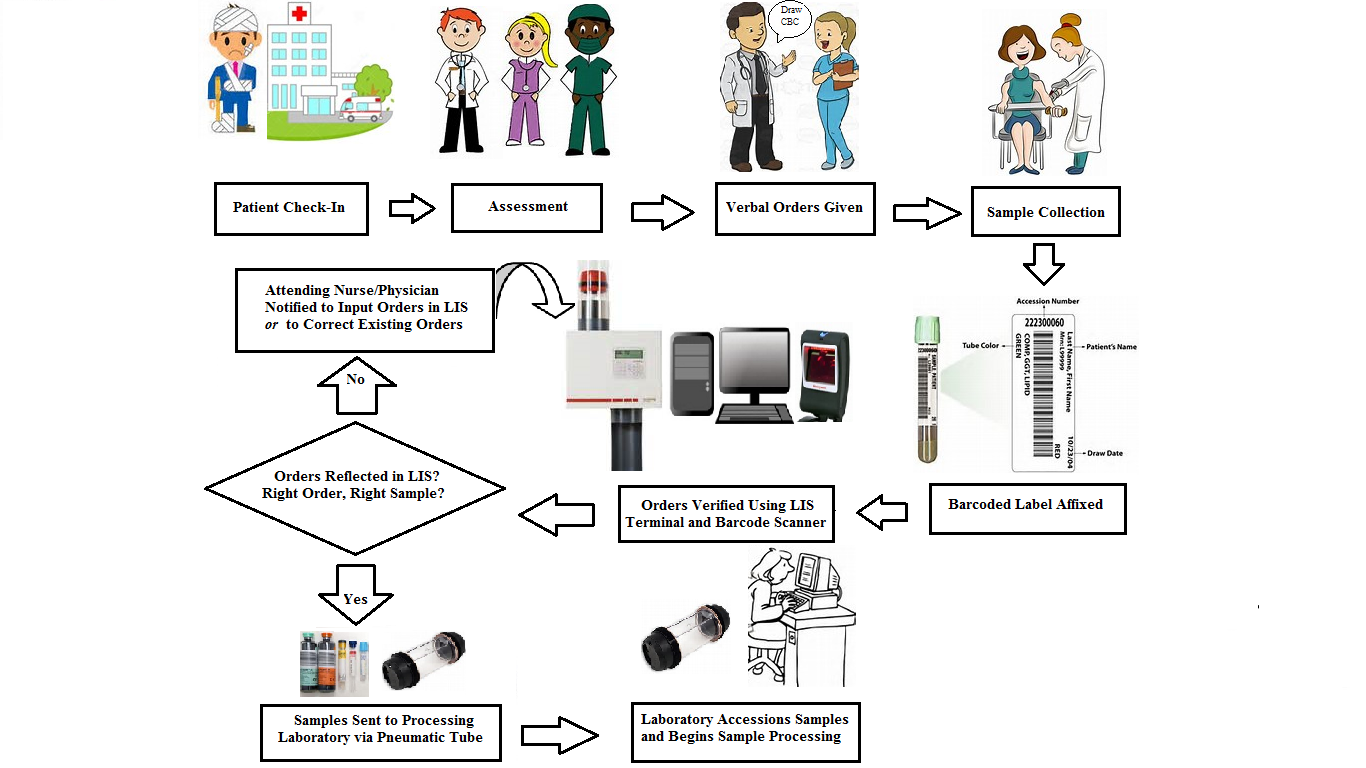
Figure 1: Flow Chart–with Barcode Scanner and LIS terminal

Figure 2: Flow Chart Sample Processing
Delivering a high-quality product at a reasonable price is not enough anymore.
That’s why we have developed 5 beneficial guarantees that will make your experience with our service enjoyable, easy, and safe.
You have to be 100% sure of the quality of your product to give a money-back guarantee. This describes us perfectly. Make sure that this guarantee is totally transparent.
Read moreEach paper is composed from scratch, according to your instructions. It is then checked by our plagiarism-detection software. There is no gap where plagiarism could squeeze in.
Read moreThanks to our free revisions, there is no way for you to be unsatisfied. We will work on your paper until you are completely happy with the result.
Read moreYour email is safe, as we store it according to international data protection rules. Your bank details are secure, as we use only reliable payment systems.
Read moreBy sending us your money, you buy the service we provide. Check out our terms and conditions if you prefer business talks to be laid out in official language.
Read more