Daniel J Lee,†* Nathan S Consedine,‡ and Benjamin A Spencer†
Author information ► Copyright and License information ►
The publisher’s final edited version of this article is available at Urology
See other articles in PMC that cite the published article.
To examine the effect of race/ethnicity and fear characteristics on the initiation and maintenance of DRE screening.
533 men from Brooklyn, NY, aged 45–70, were classified into four race/ethnic groups: US-born whites, US-born African-American, Jamaican, and Trinidadian/Tobagonian. Participants recorded the number of DRE’s in the past 10 years. Demographics and structural variables, as well as prostate cancer worry and screening fear were measured with validated tools.
Overall, 30% of subjects reported never having a DRE and 24% reported annual DRE’s. African-American, Jamaican, and Trinidadian/Tobagonian men have higher prostate cancer worry and screening fear scores than white men (all p<0.05). African-American, Jamaican, and Trinidadian/Tobagonian men were less likely to maintain annual DRE’s than white males (ORs = 0.17, 0.26, and 0.16, respectively, all p<0.05). Men with low screening fear were more likely to have an initial DRE (OR=2.3, p<0.05 vs. high screening fear), but no more or less likely to have annual DRE’s. Having a regular physician, comprehensive physician discussion, and annual visits were also associated with undergoing DRE.
We identified several ethnically-varying barriers and facilitators to DRE screening. African-American and Afro-Caribbean men undergo DRE less often and have higher prostate cancer worry and screening fear scores than white men. Screening fear predicts the likelihood of undergoing an initial, but not annual, DRE screen. Access to a physician and annual visits facilitate DRE screening. Interventions that include both culturally-sensitive education and patient navigation, and consider whether patients should be initiating or maintaining screening, may facilitate guideline-consistent screening.
Keywords: digital rectal examination, African-American, Caribbean, race, screening, prostate cancer, screening fear
African-American men face a disproportionately high burden of prostate cancer; they have 60% higher incidence and two-fold higher mortality than American-born whites.1 Caribbean men of African descent have among the highest incidences of prostate cancer in the world. In Jamaica, prostate cancer incidence rates may be as high as 304 per 100,000 men, compared to 272 per 100,000 among African-American men in the U.S.2, 3 In Tobago, the incidence rate among men aged 50–79 years was found to be 15.1%.4, 5
Several factors have been suggested to account for disparities in prostate cancer incidence and mortality, 6–9 and differences in screening practices may also contribute. With the results of the European Randomized Study of Screening for Prostate Cancer and the Prostate, Lung, Colorectal and Ovarian Cancer Screening Trial,10, 11 the American Urological Association recommended that men 40 years and older with a life expectancy of at least 10 years be offered an initial digital rectal examination (DRE) and PSA test to establish a baseline, with the decision to proceed to biopsy determined after consideration of all the patient’s individual risk factors.12 DRE’s remain an important factor in the assessment of prostate cancer risk and are independently predictive of prostate cancer.13, 14 A few data suggest that African-American and Afro-Caribbean men are less likely to undergo DRE screening than white men, even after adjusting for socioeconomic status, access to care and comorbidities.15–18
Low prostate cancer screening has been associated with lower socioeconomic status, lack of insurance, less prostate cancer knowledge, and weaker physician recommendation.19–22 Fear and anxiety related to prostate cancer and the screening process may also represent key barriers that are potentially modifiable. While men may undergo screening as a result of their decreased cancer worry, they may also avoid screening to avoid an unfavorable diagnosis or because of fear or embarrassment regarding the test itself, especially with DRE.23
Little is known about prostate screening over time, much less among African-American or Afro-Caribbean communities. It is unclear whether the low screening rates in these high-risk populations exist because men never to get an initial screening or because they fail to maintain screening patterns over time; most other studies analyze screening as a single time point. The current report examines barriers to the initiation and maintenance of DRE screening among African-American and Afro-Caribbean men, paying particular attention to the possible influence of screening fear and prostate cancer worry on DRE screening initiation and maintenance.
Five-hundred and thirty-three men living in Brooklyn, NY aged 45 – 70 participated in the study. We utilized stratified cluster sampling. We identified census tracts containing at least 25% black or white males according to the 2000 Census files, stratified them according to household income, and ordered them within income category by percentage of black and white residents. Geographically-representative numbers of black and white men in each tract were selected and trained interviewers recruited men who met the study criteria for a “Men’s Health Questionnaire Study.”
Approval for this study was obtained from the Institutional Review Boards of Columbia University and Long Island University. Data were collected from 2004 to 2006. After written consent was obtained, face-to-face interviews were conducted. Participants were paid $50 to cover time and travel expenses.
Background variables included age, race/ethnicity, relationship status, income, and education. Age, income, and education were stratified into five categories (see Table 1). For the regression models, age was analyzed as a continuous variable. The four race/ethnic groups were US-born Caucasian, US-born African-American, Jamaican, and Trinidadian/Tobagonian. Relationship status was modeled as a dichotomous variable: married/stable relationship versus single/divorced/widowed.
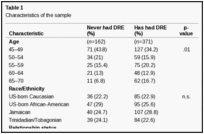
Characteristics of the sample
Health insurance status was categorized as “no insurance,” “Medicare,” “Medicaid,” or “private.” Participants completed a six-item scale assessing barriers to the use of the health care system, with their scores aggregated to form a perceived barriers measure and then analyzed as a binary variable of high vs. low health care system barriers on the basis of a median split (α = 0.66). The six questions were as follows: 1. “the health care system was not designed to be conveniently used by people like me,” 2. “I feel that I need assistance with accessing or making appointments for health care,” 3. “I don’t think that it is difficult to get reliable and professional medical care,” 4. “I have no problem dealing with the health care system,” 5. “I feel that finding a doctor is too hard for me,” 6. “I have no confidence in my ability to successfully use the health care system – either for screening or treatment processes.”
Participants reported clinical information and whether they had a regular physician, a discussion with their physician regarding prostate cancer, a positive family history of prostate cancer, or an annual physical examination. They were asked whether their physician had ever recommended prostate cancer screening and discussed their family history of prostate cancer or risk of prostate cancer. In the logistic regression model, these last three items were summed to create an aggregate measure (α=0.80) and analyzed as a binary variable of “comprehensive physician discussion” versus “non-comprehensive physician discussion.”
A prostate knowledge questionnaire was developed based on prior work and expanded in consultation with expert oncologists and urologists.17 The score consisted of 50 items evaluated by experts as belonging to six categories of prostate cancer knowledge: anatomy, screening, risk factors, warning signs, treatment, and general knowledge. These items were summed and analyzed as a binary variable of high prostate cancer knowledge versus low knowledge in the multivariate predictive models.
Participants recorded the number of DRE and PSA tests they had undergone in the past 10 years. The two screening modalities are being evaluated separately, and the results with PSA testing were previously published.19 By combining these data together with the age at which guidelines suggested they should initiate screening (varies ethnically), participants were categorized as: annual, less than annual, and never screeners.
Two different sources of fear were analyzed: fear of screening and prostate cancer worry. Fear of screening was evaluated with a five-item scale with participants answering questions like “I worry that screening procedures will hurt me somehow” and “I am afraid of prostate cancer screening” (α=0.79). Prostate cancer worry was evaluated with a five-item scale (α=0.65) which was developed from prior work on breast cancer worry among African Americans.24 Responses to the prostate cancer worry and screening fear scales were each dichotomized as high/low.
We used simple proportions with Chi-square significance testing to describe the sample. Multivariate ANOVA was used to evaluate differences in fear-related variables between racial/ethnic groups (see Table 3a) and between different DRE screening categories (see Table 3b). Logistic and multinomial regressions were used to model predictors of DRE screening practices (see Table 4). An initial binomial logistic regression was used to compare men who had never had a DRE with those who reported at least one DRE in the past ten years (“ever”). Because of our interest in the variables differentiating initiation versus maintenance profiles, we performed two multinomial regressions to distinguish 1) those who never had DRE screening from those who have DRE screening less than annually (initiation), and 2) less-than-annual screeners from annual screeners (maintenance). The first multinomial regression defined men who had never had a DRE as the referent group, represented in two different comparisons: Comparison 1 (ever vs. never) and Comparison 2 (less than annual vs. never). The second multinomial model defined less-than-annual screeners as the referent and is represented as Comparison 3 (annual vs. less than annual). Both multinomial models were designed with odds ratios greater than one representing more favorable outcomes.

Fear characteristic scores by ethnicity (a) and frequency of DRE screening (b) (Mean +/− S.D.)
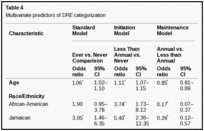
Multivariate predictors of DRE categorization
Table 1 presents the demographic characteristics of the 533 participants in our study. The average age of the cohort was 54.5 ± 7.5 years. By design, there was nearly equal representation among the four race/ethnic groups. Sixty-six percent of the men had a high-school education or less, with a median annual income between $30,000 and $49,999. More than 80% of the men had some type of medical insurance, a personal physician, and annual examinations.
Overall, 30% of the men never had a DRE. Compared to those who have had a DRE, men who never had a DRE were less likely to have a regular physician (8% vs. 39%), insurance (7.3% vs. 24%), and less likely to have had a discussion with their physician about their family history of prostate cancer, personal risk for developing prostate cancer, and recommendations for screening (all p<0.01). Two-thirds of the men who never had a DRE had a high health care barriers score, compared to 40.7% of those who have had a DRE (p<0.01).
Overall, 31% of the men reported never having had a DRE (see Table 2). White males were almost twice as likely to have annual DRE (35.5%) than African-Americans (16.9%). Men from Trinidad/Tobago had the lowest total number of DRE (2.0) screenings in the ten-year period. A subset analysis was performed to evaluate the contingency variables for the relation between DRE and PSA screening. Overall, between 57–71% of the men within each ethnic group reported having both DRE and PSA screening together. African-Americans were more likely to report only DRE’s than the other ethnic groups.
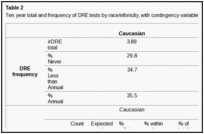
Ten year total and frequency of DRE tests by race/ethnicity, with contingency variables for the relation between DRE and PSA
African-Americans reported the highest screening fear scores (2.04) among the four groups (p<0.05, see Table 3a). African-American, Jamaican, and Trinidadian/Tobagonian men had significantly higher levels of prostate cancer worry (2.43, 2.40, 2.47, respectively) than white males (2.21, p<0.05). Fear of screening scores were also higher for African-American, Jamaican, and Trinidadian/Tobagonian men (2.04, 1.97, 1.92, respectively) than white males (1.63, p<0.01).
Men who never had a DRE had significantly higher fear of prostate screening scores (2.21) than those who had annual (1.64, p<0.05) and less than annual (1.82, p<0.05, see Table 3b) DRE. Prostate cancer worry scores were higher for men how never had a DRE (2.53) than those who had less than annual (2.32) or annual (2.30, p<0.05) exams.
Relative to those who never had a DRE (Comparison 1 or Standard Model), men were less likely to have ever had a DRE if they did not have a regular physician (OR=0.33, 95% CI: 0.17–0.64), did not have an annual examination (OR=0.45, 95% CI: 0.25–0.82), and did not have a comprehensive discussion with their physician (OR=0.38, 95% CI: 0.23–0.62, see Table 4). Those with low screening fear were more likely ever to have had a DRE than those with high screening fear (OR=2.7, 95% CI: 1.5–4.8).
The Initiation model (Comparison 2) compared the odds of having less-than-annual DRE screenings to never having had a DRE. African-American (OR=3.7, 95% CI: 1.73–8.1), Jamaican (OR=5.4, 95% CI: 2.4–12.4), and Trinidadian/Tobagonian males (OR=6.3, 95% CI: 2.8–14.4) were more likely to have DRE screenings less than annually compared to white males. Men without a regular physician (OR=0.35, 95% CI: 0.17–0.70) and those who reported a non-comprehensive physician discussion (OR=0.39, 95% CI: 0.23–0.66) were less likely to be in the less than annual DRE group than the never screened group. Those with low screening fear (OR=2.35, 95% CI: 1.29–4.28) had more than 2 times the odds of having less than annual DRE screenings than never having a DRE.
In the Maintenance model (Comparison 3), we evaluated the odds of having annual DRE’s to having less-than-annual DRE’s. Each additional year of age was associated with a 15% decrease in the odds of maintaining annual DRE (OR=0.85, 95% CI: 0.81–0.89). African-American (OR=0.17, 95% CI: 0.07–0.37), Jamaican (OR=0.26, 95% CI: 0.12–0.57), and Trinidadian/Tobagonian males (OR=0.16, 95% CI: 0.07–0.36) were less likely to maintain annual DRE screenings than white males. Men who did not have annual physical examinations were also less likely to have annual DRE screenings (OR=0.30, 95% CI: 0.11–0.80).
No prior study has evaluated the effect of fear on the initiation and continuity of DRE’s among Afro-Caribbean sub-populations. After controlling for ethnicity and other demographic factors, men with low screening fear had 2.4 times the odds of initiating a DRE screening (versus not screening) compared to those with high screening fear. However, once high screening fear men had undergone at least one DRE, they were just as likely to maintain annual DRE’s as those with low screening fear. Prior work by Consedine et al17, 25 found that fear of screening, especially embarrassment and discomfort regarding DRE’s, is a significant barrier to prostate cancer screening, while prostate cancer worry is a facilitator to screening. Concern and worry may follow a bimodal distribution: moderate levels may promote health behaviors, while high levels promote denial and avoidance.17, 26 Importantly, these fear and worry characteristics varied across the ethnic groups. Overall, African-American and Afro-Caribbean men had significantly higher prostate cancer worry and screening fear than the white males. Trinidadian/Tobagonian men had the highest prostate cancer worry levels, while African-American men had the highest screening fear levels. These finding are consistent with other studies suggesting that men from minority populations have high levels of worry about prostate cancer and are particularly averse to DRE testing.17, 27, 28 DRE’s have unique psychological demands for men which may be intensified given the similarities between the test itself and the disease for which it is screening regarding issues of vulnerability, humiliation, and sexuality.7, 17
Another important finding of the study is the importance of ethnicity in DRE screening behavior. African-American, Jamaican, and Trinidadian/Tobagonian men had significantly fewer DRE screenings than white males, confirming the findings of several other studies.15, 17, 18 African-American and Afro-Caribbean men were between 74% and 84% less likely to maintain annual DRE screenings, similar to the PSA screening behavior that Gonzalez et al19 found in the same study cohort. PSA testing is often done in conjunction with DRE screenings, however PSA screening does not share the same complex relations with fear and anxiety as DRE screening.17 Men from these three specific sub-populations reported similar trends in prostate cancer screening, prostate cancer worry and screening fear; however, the appropriate clinical intervention to address these fears may be very different for each culture. Hispanic, African-American, and Caribbean communities exhibit diversity in cultural and healthcare practices.17 Therefore, more research is necessary to clarify the risk-profiles of each community and the best means to address the existent disparities in care.
Finally, this study suggests that physician-patient interactions may be more influential in facilitating the initiation of DRE screening versus engendering a maintenance pattern. Prior studies found that those who did not have a consistent source of health care had lower screening rates.18, 29 In this cohort, men who lacked a regular physician or comprehensive discussions about prostate cancer were 65% and 61% less likely to initiate DRE screening, respectively, but had equivalent odds of maintaining annual DRE’s.
There are several limitations to our study. The self-reported outcomes referenced a period of ten years and are therefore subject to recall bias. Because the data are cross-sectional, the results may show correlations but do not reveal causality. Finally, the participants were all men living in Brooklyn, New York and therefore the findings may not apply to all Afro-Caribbean and African-American populations in the United States.
Despite major advances in prostate cancer detection and treatment, there remains a large disparity in screening utilization rates among men at higher risk of dying from prostate cancer. Several ethnically-varying barriers and facilitators to DRE screening were characterized in this study. African-American and Afro-Caribbean men undergo DRE less often and have higher prostate cancer worry and screening fear scores than white men. Screening fear predicts the likelihood of undergoing an initial, but not annual, DRE screen. Access to a physician and annual visits facilitate DRE screening. Interventions that include both culturally-sensitive education and patient navigation, and consider whether patients should be initiating or maintaining screening, may facilitate guideline-consistent screening.
In a quantitative study that utilized stratified cluster sampling in order to identify barriers and facilitators to digital rectal examination screening among African-American and Afro-Caribbean men, Lee, Consedine, and Spencer (2011) identified that while screening fear predicts the likelihood of undergoing initial screening, it does not predict the likelihood of undergoing an annual DRE screen. This was attributed to having a regular physician who engaged in comprehensive and culturally-sensitive discussion on the important and benefits of screening, thereby encouraging African-American and Afro-Caribbean men to undergo annual screening. The discovery was an optimistic one, therefore, because it was suggestive of a legitimate facilitative factor to cancer screening.
Another study gave regard to how an emphasis on the “perceived benefits” of cancer screening can facilitate active decisions to undergo screening processes. For instance, Tingen et al. (1998) “conducted a correlational study” in which 1,522 men were involved (72% African-American, aged 40-70 years; 28% Caucasian, aged 50-70 years). “The purpose of the study was to explore the perceived benefits as facilitators of participation in prostate cancer screening. The results indicated that men who perceived participation in prostate cancer screening as a benefit were more likely to participate in screening”. The study proved influential because it reinforced the notion that knowledge of, and active education on, prostate cancer is a likely facilitator to ongoing participation in screening.
OTHERS TO REVIEW
Oncol Nurs Forum. 1998 Apr;25(3):527-34.
Weinrich SP1, Weinrich MC, Boyd MD, Atkinson C.
To test the effect of knowledge on participation in prostate cancer screening.
Quasi-experimental design; PRECEDE framework.
319 men, 82% African American.
Prostate cancer knowledge was measured with a Prostate Cancer Knowledge Questionnaire prior to a community-based educational program. Men were referred to their personal physicians for a free prostate cancer screening. Results were sent to the Prostate Cancer Project.
Prostate cancer knowledge and participation in free prostate screening with a digital rectal examination and prostate specific antigen.
Prostate cancer knowledge was a predictor in participation in screening (p = 0.05).
Nurses need to target educational interventions for African American men, who have the highest incidence of and mortality rates for prostate cancer, to significantly reduce mortality rates. This study documented the importance of providing educational programs to increase participation in prostate cancer screening.
PMID:
9568607
[PubMed – indexed for MEDLINE]
Oncol Nurs Forum. 1995 Sep;22(8):1253-5.
Gelfand DE1, Parzuchowski J, Cort M, Powell I.
To explore the relationship between attitudes toward digital rectal examination (DRE) and participation in prostate cancer screening among African American men.
Survey.
Prostate cancer screenings with a prostate-specific antigen (PSA) blood test held at churches with African American members in Detroit, MI.
613 African American men between the ages of 40 and 70.
Self-administered, structured questionnaires examining attitudes toward DRE, past experiences with DRE, and fear of cancer.
Willingness to undergo DRE.
The majority of men who were screened had positive attitudes about DRE. Fear of cancer was associated with negative attitudes toward DRE. DREs were not a deterrent among men who attended the screenings.
Negative attitudes toward DRE do not necessarily deter African American men from participating in prostate cancer screenings.
Prostate cancer screening programs should attempt to use both DRE and PSA. More reliable prostate cancer indicators are obtained by incorporating DRE with PSA tests.
PMID:
8532550
[PubMed – indexed for MEDLINE]
J Natl Med Assoc. 2006 Apr; 98(4): 515–519.
PMCID: PMC2569232
Satoshi Anai, John Pendleton, Peter Wludyka, Christopher Williams, Leah Nelms, Curtis Pettaway, and Charles J. Rosser
Author information ► Copyright and License information ►
This article has been cited by other articles in PMC.
CONTEXT: In the era of serum prostate-specific antigen (PSA) screening, the incidence of prostate cancer has increased dramatically. Simultaneously however, stage migration has occurred, and treatment outcomes have improved. Inner-city men have lower screening rates and, thus, may be diagnosed with more advanced disease that it less likely to be successfully treated. OBJECTIVE: To assess the detection rate of prostate cancer and tumor stage at presentation in inner-city men. DESIGN, SETTING, AND PATIENTS: A retrospective cohort of 368 men underwent transrectal ultrasound needle-guided biopsy at an inner-city hospital from January 2003 to May 2005. Clinical and pathologic data were collected and analyzed. MAIN OUTCOME MEASURES: Clinic and hospital records were reviewed for several key outcomes, including prostate cancer incidence, tumor stage and tumor grade. RESULTS: The median age of the cohort was 67 +/- 9.1 years (range, 23-93 years). Prostate cancer was diagnosed in 44% of subjects (161/368). The median PSA level at the time of diagnosis was significantly higher in African-American men than in Caucasian men (9.82 vs. 5.97 ng/mL, P=0.008). Abnormally high serum PSA levels (>20 ng/mL) were present in disproportionately more African-American men than Caucasian men with prostate cancer (32.9% vs. 19.7% P=0.011). African-American men in this inner-city cohort also had a higher incidence of advanced disease or distant metastasis (T3/T4, N1, or M1) than did Caucasians (16.1% vs. 3.8%; P=0.045). CONCLUSIONS: Compared with inner-city Caucasian men, disproportionately more inner-city, African-American men present with advanced prostate cancer. This observation warrants prostate cancer education and consideration of early detection programs in underserved inner-city communities.RELATED: http://www.ncbi.nlm.nih.gov/pubmed?itool=pubmed_Abstract&DbFrom=pubmed&Cmd=Link&LinkName=pubmed_pubmed&IdsFromResult=16585144&retmode=ref
Delivering a high-quality product at a reasonable price is not enough anymore.
That’s why we have developed 5 beneficial guarantees that will make your experience with our service enjoyable, easy, and safe.
You have to be 100% sure of the quality of your product to give a money-back guarantee. This describes us perfectly. Make sure that this guarantee is totally transparent.
Read moreEach paper is composed from scratch, according to your instructions. It is then checked by our plagiarism-detection software. There is no gap where plagiarism could squeeze in.
Read moreThanks to our free revisions, there is no way for you to be unsatisfied. We will work on your paper until you are completely happy with the result.
Read moreYour email is safe, as we store it according to international data protection rules. Your bank details are secure, as we use only reliable payment systems.
Read moreBy sending us your money, you buy the service we provide. Check out our terms and conditions if you prefer business talks to be laid out in official language.
Read more