A PHENOMENOLOGICAL INQUIRY
DISSERTATION PROPOSAL
Presented in Partial Fulfillment of the
Requirements for the Degree of
Doctor of Philosophy in Nursing
THE LIVED EXPERIENCE OF JAMAICAN MEN IN THE US WHO HAVE UNDERGONE PROSTATE CANCER SCREENING: A PHENOMENOLOGICAL INQUIRY
DISSERTATION PROPOSAL
All Rights Reserved
Background: The US ranks among top five nations with Prostate Cancer (PCa) fatalities, with the highest number of fatalities occurring in African and Caribbean immigrant populations. Jamaican men constitute a high-risk population for PCa incidences and they are least likely to undergo prostate cancer screening or follow up with subsequent screening.
Purpose: The proposed phenomenological study seeks to understand how Jamaican men ascribe meaning based on their experiences after undergoing PCa screening sessions. Method: The researcher will use hermeneutic phenomenology guided by van Manen’s (1990) framework to collect and analyze the primary data. The target population for the study will be Jamaican men living in South Florida who have already undergone PCa screening. A purposive sampling sample of the Jamaican men will be recruited using a referral sampling procedure within the Jamaican community in South Florida. Qualitative data will then be collected using face-to-face interviews, and the participant interviews will continue until emergent themes and contextual categories are saturated.
Results and Conclusions
Pending
CHAPTER ONE: INTRODUCTION TO THE STUDY 1
PROBLEM AND DOMAIN OF THE INQUIRY 1
Prostate Cancer: Global Incidence and Prevalence 1
Prostate Cancer in the Caribbean and Jamaica 4
Prostate Cancer in the United States 7
PCa Screening: A Tale of Two Decisions 9
Experiences Prior, During and After Prostate Cancer Screening 10
Philosophical Underpinnings 13
Interpretivism Paradigm: Constructivist Approach 13
Qualitative Research Methodology 17
Philosophical Assumptions of Qualitative Research 19
Phenomenology for this Study ………………….……….…………31
Significance of the Study to Nursing 33
Implications of the Study to Nursing Education 34
Implications of the Study to Nursing Practice 35
Implications of the Study to Nursing Research 36
Implications of the Study to Health/Public Policy 38
Scope and Limitations of the Study 39
CHAPTER TWO: REVIEW OF LITERATURE 41
Historical Context of PCa Screening 43
Prostate Cancer Risks in the Globe, Caribbean, Jamaica, and the United States 43
Jamaican Men in United States and Prostate Cancer Risks 46
Prostate Cancer Screening as an Intervention Measure 48
Geographical and Social Profile of Population under Study: Jamaica Men 50
Previous Research on PCa Screening among Jamaican Men 52
Research on Experience, Adherence, and Impact of PCa Screening 54
Researcher’s Experimental Background, Involvement, Experience and Interests 59
Use of Reflexivity and Bracketing 60
Appropriateness of Research Design 62
CHAPTER THREE: RESEARCH METHODS AND METHODOLOGY 65
Qualitative Research Methodology 65
Research Design: van Manen’s (1990) Model of Hermeneutic Phenomenology 66
Diagrammatic Presentation of the Research Design 69
Research Sample and Setting 71
Access and Recruitment of the Sample 73
Final Sample Size and Justifications 73
Ethics and Ethical Considerations 74
Protection of Human Subjects 74
Participants’ Informed Consent 74
Privacy and Confidentiality 75
Data Collection Process and Procedures 75
Credibility of Research Findings 81
Dependability of Research Findings 82
Confirmability of Research Findings 83
Transferability of Research Findings 84
Appendix A: Sample of Face-to-Face Interview Questions 98
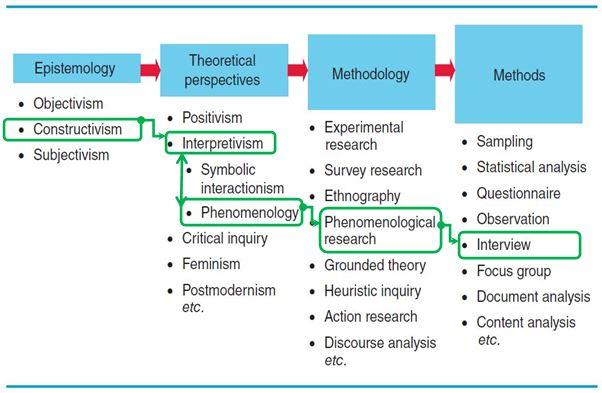
Figure 1. The paradigmatic schema (Foster, S. 2016, adapted from Crotty, 1998 with modifications). 17
Figure 2. The hermeneutic research design (Foster, S. 2016, adapted from van Manen, 1990 with modifications) 66
Prostate cancer (PCa) incidence rates are the highest globally among Jamaican men, yet these men are the most likely to attend such a preventative and control measure as PCa screening (Consedine, Adjei, Horton, Joe, Borrell, Ramirez & Neugut (2009). There is an overwhelming body of evidence linking Jamaican men and non-adherence to PCa screening (Ajzen, 1991; Consedine et al., 2009; Edelstein & Gillath, 2008; Evans, Butler, Etowa, Crawley, Rayson & Bell, 2005). Much is known about Jamaican men’s none adherence to PCA screening, but very little is known about their experience of undergoing the screening process when they do attend. To gain an understanding of the essence of this phenomenon a qualitative phenomenological inquiry will be conducted. An understanding of how Jamaican men, who are proactive about their prostate health, make meaning of the experience of undergoing prostate cancer screening, may facilitate the development of more effective interventions targeting the group’s overall rates of prostate cancer screening.
The prostate gland is only found in males, and according to the American Cancer Society (2015), it functions to produce a protective and nourishing liquid for sperm cells in the semen. Prostate Cancer (PCa) is the development of cancerous cells alongside natural body cells in the prostate gland, through a process referred to as adenocarcinoma (American Cancer Society, 2015). As such, the male gender is the exclusive population at risk of developing the PCa condition, and the risk often starts at the middle age of 40, and worsens as a man ages towards the age of 80 years. Today, PCa is “the second most common cancer in men,” in the world (Globocan, 2015, p. 1).
The study will focus on PCa screening, which according to Dowdle (1999), is a clinical procedure aimed at diagnosing the presence of any cancerous cells in the prostate gland. Today, numerous researchers, practitioners and scholars including Gibson, Hanchard, and Waugh (2010), Aiken, Tulloch, Freeman, Bennett, Coard, Panton and Flanigan (2003), and Haas, Delongchamps, Brawley, Wang and De la Roza (2009) have published research findings that qualified PCa screening as an effective diagnostic tool when controlling PCa. Further, according to Dowdle (1999), controlling, eradicating and preventing Prostate Cancer (PCa) relies on several factors including: (a) how informed health care programs are about PCa, (b) what is known about PCa, (c) appraisal of available interventions against PCa, and (d) accurate characterization of specific populations respond to PCa
The PCa screening procedure helps detect any cancerous cells in the testicles. Screening enables health care providers “discover clinically significant disease early in the disease process to prevent mortality and morbidity through treatment” (Aiken & Eldemire-Shearer, 2012, p. 90). The International Agency for Research on Cancer commends screening is the most effective and reliable PCa control strategies, mainly because screening enables early diagnosis and successful treatment (Globocan, 2015). PCa screening is justified as both requisite and appropriate. According to Catalona, Loeb and Han (2006), PCa screening helps determine the presence of cancerous cells when the condition is in its early stages.
The World Health Organization (WHO) reported that over 15,296,000 men died of cancer between 2007 and 2012 (Globocan, 2015).The International Agency for Research on Cancer (IARC) reported on behalf of the WHO, and affirmed that in 2012, the world registered over 14,068,000 new cases of cancer (incidences), formally diagnosed and triggering the deaths of 4,653,000 men (Globocan, 2015). In a journal article published for clinicians on global cancer statistics, Jemal, Bray, Center, Ferlay, Ward and Forman (2011) noted that, the global incidence risk for all types of cancer was 30% in developed nations and 17% in less developed nations (at Age-Standardized Rate per 100,000 of 300.1). Further, the global mortality risk for all types of cancer was 15% in developed nations, and 17% in less developed nations (at Age-Standardized Rate per 100,000 of 160.3). Importantly for the present study, Jemal et al. (2011) established that among all cancers, PCa incidence risk was the highest, at 7.8% in developed nations, and only 2.5% in less developed nations (at Age-Standardized Rate Per 100,000 of 62.0). Finally, among all cancers, PCa mortality was the highest, at 1.2% in developed nations (at Age-Standardized Rate per 100,000 of 12.0) (Jemal et al. 2011, p. 73)
PCa is regarded as the most sensitive type of cancers among men globally, based on the annul number of incidences and mortalities recorded. Nearly a decade ago, Garcia, Jemal, Ward, Center, Hao Siegel and Thun (2007) reported that over 782,600 new cases of PCa were recorded, triggering over 254,000 deaths, globally. According to Garcia et al. (2007), PCa had become the sixth leading cause of cancer death among men across the globe, by 2007. What Garcia et al. (2007) did not anticipate at the time was that though the trend had worsened by 2007, the rise was only a start point, and PCa risk would become more catastrophic by 2010 (Jemal, Center, DeSantis & Ward, 2010, p. 1899).
Important for the present study is the consequent impact of PCa among men, globally. As affirmed by Sinfield, Baker, Agarwal, and Tarrant (2008), based on statistics, PCa patients recorded the worst experiences compared to the experiences recorded with other type of cancers including breast and stomach cancers. The foregoing reality, alone, prompts urgent review of the resultant experiences from PCa, and in this study specifically, PCa screening. Prior to further discussion of that, however, it is important to highlight PCa risks and mortality trends by race and ethnicity, as well as by nationality, above the foregoing global trends.
Between 1999 and 2012, the Centers for Disease Control and Prevention (2015) reported that, “the rate of men dying from prostate cancer has varied, depending on their race and ethnicity,” where Caribbean and Black/African men record the highest PCA mortality rate. According to CDC, the PCa incidence/mortality rate was significantly influenced by both race and ethnicity, since “black men had the highest rate of getting prostate cancer, followed by white, Hispanic, American Indian/Alaska Native men, and Asian/Pacific Islander” (¶p. 1). The PCa incidence and mortality rate categorized Caribbean men under the same profile as men with African descent. Based on PCa incidence, prevalence, and mortality rates recorded in the Caribbean nations by 2008, it soon emerged that Caribbean men, alongside African men, had the highest recorded risk of developing PCa cancer. Consequently, compared to any other region in the world, the Caribbean region alone triggers the highest number of PCa incidences every year (Prostate Cancer Caribbean, 2008).
Aiken and Eldemire-Shearer (2012) conducted a study on the role of PCa screening to intervene against the rising mortality trends in Jamaica and the wider Caribbean. In the study, the researchers reported that of greater concern in the rising PCa incidence statistics globally is the indication “that the Caribbean region has the highest age-standardized PCa-specific mortality rate in the world at 26.3/100 000/year” (p. 90). The racial profile of black and Caribbean men triggers a genetic weakness that is at a higher risk of developing PCa compared to all other racial profiles (Glover, Coffey, Douglas, Cadogan, Russell, Tulloch, & Walsh, 1998). Aiken and Eldemire-Shearer (2012) highlighted the increasing concern of Jamaica’s rising PCa incidences and mortalities, which are already extremely high given “that the Caribbean region has the highest age-standardized PCa-specific mortality rate in the world” (p. 90).
In agreement, Gibson, Hanchard, and Waugh (2010) reported that Black and Caribbean populations have the highest risk of developing PCa in the world. A similar trend is notable in the Jamaican nation as part of the Caribbean. Prostate Cancer Caribbean (2008) reported that, in the Caribbean region, cancer incidences registered nationally in Jamaica, the Bahamas, Cuba, Trinidad and Tobago, Grenada, and Martinique have qualified the Caribbean as one of the most high-risk locales of PCa. Knowing that Jamaican men, alongside the Caribbean and Black men have the highest PCa incidence and mortality rates would perhaps not be as worrisome to clinicians if something effective was being done about it. After reviewing what this high-risk population is doing to intervene against preventable deaths, clinicians, nurses, and medical scholars/researchers are worried about what is being done. As argued by Aiken and Eldemire-Shearer (2012), “if PCa is identified early in its natural history, it is eminently treatable with great potential for cure” (p. 90). As such, since “the Caribbean has the highest age standardized PCa-specific mortality rates in the world,” then “why is this so and what can be done to reduce the morbidity and mortality associated with PCa in the Caribbean?” (p. 90).
Many previous studies have conclusively established the high risk of developing PCa among Jamaican men, most notably Aiken and Eldemire-Shearer (2012), and Gibson, Hanchard and Waugh (2010). Traditionally, “the highest reported incidence of prostate cancer in the world was thought to be among American Black men¸” and no study focused on the Caribbean immigrants (Glover et al., 1998). However, statistics eventually showed that the incidence rate in the Jamaican capital, Kingston alone, reached 304/100,000 men, 80% of whom were pathologically confirmed. A higher risk value was identified among Jamaicans in Jamaica, that in African men, with 30% of the patients having “acute urinary retention, 16% presented with bone metastases, 15% with gross hematuria at the time of diagnosis and 42% with an abnormal rectal examination suspicious for cancer” (Glover et al., 1998, p. 1984). Importantly, Prostate Specific Antigen (PSA) measures among Jamaican men diagnosed 7% of the PCa cases in 1989 and reached “48% of cases by 1994” (p. 1984).
Gibson, Hanchard, and Waugh (2010) reported that black and Caribbean populations have the highest risk of developing PCa in the world. Gibson, Hanchard and Waugh (2010) argued that, based on incidences reported between 2003 and 2007, PCa is “the leading cancer affecting men in Jamaica” (p. 456). In agreement, the American Cancer Society (2008) reported that Jamaican men have a high risk of developing PCa among comparable racial profiles. Many other research studies established the high risk of developing PCa among Jamaican men. According to Aiken and Eldemire-Shearer (2012), Jamaica represents the region of the Caribbean territories with the highest rates of PCa.
Morrison, Aiken, and Mayhew (2014) reviewed the “current state of prostate cancer treatment in Jamaica” (p. 456). The researchers reported that in Jamaica today, PCa “accounts for almost a third of all cancers diagnosed” with Jamaica having “the highest incidence of PCa in the world, based on a reported rate of 304/100,000 per year” (p. 456). Further, according to records by the Jamaica Cancer Registry, PCa “is the most common cancer overall as well as the most common cancer in men” with an “age-standardized incidence rate of 78.1/100,000 per year” (Morrison, Aiken, & Mayhew, 2014, p. 456). It is of greater concern that by 2014, PCa was “the most common cause of male cancer-related deaths, with an age-standardized mortality rate of 53.9/100,000 per year” (Morrison, Aiken, & Mayhew, p. 456).
The fact that PCa incidence and mortality rates are the highest among African and Caribbean Black men, an ethnic profile in which Brazilian men belong, can easily but wrongly signify Jamaica as ground zero of PCa research and PCa screening. The proposed study will employ the “racial and ethnic profile” of men when defining their PCa incidence and mortality rates and linking such trends with screening experiences. Besides being in Africa and Caribbean region, the racial profile amplifies the PCa incidence and mortality rate. This means that, the high risk of developing PCa affects not only Jamaicans within Jamaica, but also those who have immigrated to the U.S.
According to Kendrick (2010), “research has shown that prostate cancer is the second leading cause of cancer death among men in the United States and Caribbean and African American men are more likely to develop the disease than White American males” (p. 6). Jamaican men residing in the U.S. thus depict a similar high PCa risk as those in Jamaica. The American Cancer Society (2008) and Gibson, Hanchard, and Waugh (2010) established that Jamaican men have the highest rates of PCa even within the U.S., when profiled by race and ethnicity as being Caribbean.
The National Cancer Institute (NCI, 2015) initiated the Surveillance, Epidemiology, and End Results Program (SEER) under the partnership of the National Institutes of Health, the National Cancer Institute, and the U.S. Department of Health and Human Services. The SEER program focused on PCa incidence and mortality rates within the U.S., and by 2015, established the following, between 199 and 2012, 137.9 per 100,000 cases of PCa were reported annually (incidences), which triggered 21.4 per 100,000 mortalities in men per year.
On PCa prevalence by 2012, an estimated 2,795,592 men were already clinically diagnosed as living with PCa in the United States. Further, the lifetime risk for developing cancer ranges at 14% for PCa among men in their lifetime, and PCa represents over 13.3% of all new cancer cases diagnosed in the U.S. Finally, according National Cancer Institute, PCa is the third most common type of cancer diagnosed in the U.S. (NCI, 2015, p. 1-2).
The U.S. is third among all countries based on the PCa incidence and mortality rates, records these significant numbers among the Black and Caribbean males. The tragedy occurs mostly among Jamaican men, than in Black and Caribbean men. According to Glover et al. (1998), Jamaican men in the U.S., “have a high incidence of prostate cancer, much higher than even Black Americans during a similar period” (p. 1984). Notably, PCa impacts are “more significant clinically with greater morbidity” among Jamaica men that any other racial and ethnic profile (p. 1984).
The American Cancer Society (2008) established that, based on global cancer fact and figures, PCa incidences and mortalities are higher in the U.S. than in the Africa and the Caribbean, yet within the U.S., the highest rates are among the Caribbean (notably Jamaican) and African men. Kendrick (2010) established that male Caribbean immigrants to the U.S. have the highest PCa risk based on incidence rates. Further, according to the American Cancer Society (2015), the Caribbean and African-American men are twice more likely to develop PCa than men from other races, such as Asian-American, Hispanic-Latino, and non-Hispanic White men. Research has attributed the high risk to genetic factors dominant in their ethnic profiles (American Cancer Society, 2008b).The proposed study will therefore focus on the immigrant population of Jamaican men in the U.S.
PCa screening has largely been advanced as the most effective and standardized diagnostic tool and intervention strategy for PCa (Concato, Wells, Horwitz, Penson, Fincke, Berlowitz & Peduzzi, 2006; Aiken & Eldemire-Shearer, 2012). PCa screening has been characterized as having no viable competition from alternative options, being the only standardized, affordable, reliable, and effective intervention measure against the rising incidence and mortality rates of PCa. Notably, PCa is the second most common cancer in men, with Jamaican men suffering the highest rate of occurrence and mortality from this prostate malignancy (Eldemire-Shearer, James, Morris, Holder-Nevins, Lawes & Harris, 2011; Globocan, 2015). Notably, however, if not diagnosed early, PCa can quickly develop to mature and metastatic stages that are less responsive to treatment (Aiken & Eldemire-Shearer, 2012). PCa screening is commonly done using a Digital Rectal Exam (DRE) and/or a serum analysis of Prostate Specific Antigen (PSA).PCa screening has been associated with favorable prognoses, and decreased mortality, and according to Clarke et al. (2012), high-risk PCa populations should ideally record the highest adherence score.
Nonetheless, PCa screening is not without opposition, and in most parts, controversy. Several studies have disqualified PCa as an effective, even appropriate, preventative and control measure against PCa. Kilpelainen, Tammela, Maattanen, Kujala, Stenman, Ala-Opas and Auvinen (2010), Howrey, Kuo, Lin and Goodwin (2013), and Maattanen, Hakama, Tammela, Ruutu, Ala-Opas, Juusela & Auvinen (2007), faulted PCa screening for generating false PSA positives results and false negative results.
The inaccuracy of PCa screening has thus been faulted and even linked to negative impacts on people falsely diagnosed of PCa by among others Berner (2009), Howrey, Kuo, Lin and Goodwin (2013), and Onyiaorah, Onyiaorah, Ukah, Anyiam, Onwukamuche and Efobi (2015). The criticism of PCa screening has valid arguments. To exemplify, it is noteworthy that neither PCa screening procedure, the PSA and Digital Rectal Examination (DRE) procedures, are 100% accurate and only the clinical biopsy of the prostate is the definitive clinical test available (Kilpelainen et al., 2010). Yet PSA and DRE, rather than clinical biopsy are the most common, most recommended, and only feasible screening options available in many regions. This explains why there has not been any official recommendation for PCa screening agreed upon by major medical and cancer organizations (Basch, Oliver, Vickers, Thompson, Kantoff, Parnes & Nam, 2012).
Regardless of the accuracy attained by the PCa screening procedures, perhaps the most important question is what PCa screening attains or enables. The early PCa diagnosis enabled by PCa screening is not always essential in reducing morbidity and mortality. PCa is a slow-growing type of cancer, and most men die old from other causes regardless of their prostate status. This argument questions the necessity of PCa screening (Howrey et al., 2013; Onyiaorah et al., 2015). Finally, for the present discussion, PCa screening is not mandatory. As such, any such population as Jamaican men who are at a higher risk of developing PCa are not compelled or obligated to participate in screening. No policy can obligatorily require asymptomatic, healthy men to undergo early PCa screening. In question, therefore, is how effective PCa screening can be as a preventative and control measure against PCa.
Jamaican men constitute a high-risk population for PCa incidences, and most research studies identify Jamaican men as a high-risk population for PCa (Aiken and Eldemire-Shearer, 2012). It is also apparent that PCa screening presents the only formidable, reliable, and effective intervention measure that the high-risk population of Jamaican men can employ to reduce their mortality rates. It is logical to expect Jamaican men to be the most loyal supporters and most adherent to PCa screening, yet the real-life data suggests the opposite, justifying the proposed study, perhaps more than any other fact.
Evidence suggests that Jamaican men avoid PCa screening, either because they do not care or because they do not know of their high PCa risk status or the role of PCa screening. Further, most Jamaican men currently residing in the U.S. do not avoid PCa screening because the requisite screening facilities are inaccessible and services unaffordable. Rather, Jamaican men avoid PCa screening, regardless of whether the results may be positive or negative, deliberately and consciously. The question that thereof emerges, is why do Jamaican men do still avoid PCa screening.
Taitt (2015) generated adequate evidence contending that Jamaican men have a unique set of “lived experiences, perceptions, and beliefs” that influence their decisions regarding PCa screening (p. 4). Modern understanding of PCa screening in the U.S. needs to acknowledge “the perspectives, experiences, and beliefs of Afro-Caribbean men relative to prostate cancer” (Taitt, 2015, p. 199). Outside the U.S., the lived experiences of Afro-Caribbean men residing in the UK have taught them that, “it doesn’t make sense to worry too much” as to attend screenings (Nanton& Dale, 2011, p. 62). As such, whether already adequately informed or otherwise, whether PCa screening facilities are accessible, and the procedure affordable, Jamaican men perceive PCa screening based on their lived experiences. Of great concern, therefore, are Jamaican men subscribing to “misperceptions about cancer risk,” where PCa is regarded as “a taboo topic,” excluded from consideration by virtue of cultural beliefs and social norms (Friedman, Corwin, Rose, & Dominick, 2009, p. 209).
Even among Jamaican men in the U.S., PCa screening is regarded emotively, such that the decision to screen or otherwise is the outcome of emotional patterns of thought (Consedine et al., 2008). Fear of PCa, fear of undergoing the screening procedure, overwhelming anxiety, and emasculation concerns among immigrant Caribbean men in New York, influence their perception of and adherence to PCa screening (Consedine, Adjei, Horton, Joe, Borrell, Ramirez & Neugut, 2008). Therefore, the decision to undergo PCa screening among Jamaican men is the product of lived experiences as reflected by cultural, social, and economic realities (Friedman et al., 2009); fear, anxiety, concerns, and negative beliefs (Consedine et al. 2008); level of awareness (McCree-Hale, Hale, Rutley, Aung & Jolly, 2012); as well as accessibility and affordability (Aiken & Eldemire-Shearer, 2012).
PCa incidence and mortality rates of Black and Caribbean men, particularly of Jamaican men, are the highest of all other racial profiles in the world. The U.S. has the third highest national PCa incidence and mortality rates in the world, and the highest rates recorded among the Jamaican immigrant, than in any other racial profiles of U.S. immigrants. PCa screening is the only feasible, standardized, affordable, and reliable intervention and control intervention against PCa, available today. Yet despite having the highest PCa incidence and mortality rates, regardless of availability or community health efforts, Jamaican men willingly and persistently, refuse to adhere to PCa screening, because of their cultural beliefs and knowledge. Evidently, the high non-adherence level among Jamaican men has already been the point of interest for numerous studies over the last three decades, as exemplified by Ajzen (1991), Consedine et al. (2009), Edelstein and Gillath (2008), and Evans et al. (2005) and many other similar studies.
The narrow focus of previous research on non-adherence to PCa screening has neglected the experience of Jamaican men who are proactive about their prostate health. While many avoid PCa screening, some are adherent to and actively conscious of the need for screening. We now only know what influences Jamaican men to avoid PCa screening, but not what motivates some to adhere to screening, or what happens after some Jamaican men attend the screening sessions. Such scholars as Taitt (2015), Aiken and Eldemire-Shearer (2012), and Aiken, Tulloch, Freeman, Bennett, Coard, Panton & Flanigan (2003) have identified why Jamaican men avoid PCa screening, yet all remain silent about those who undergo screening. The gap of knowledge is why some, Jamaican men willingly chose to attend PCa screening, what happens after undergoing screening, how they feel after the screening, and likelihood of undergoing future screening. Given the critical essence and role of PCa screening as discussed above the present study seeks to investigate a significant phenomenon among a PCa high-risk population that willingly and deliberately opts to ignore the screening intervention.
The proposed study seeks to understand the decision that some healthy Jamaican men make to undergo early PCa and be proactive about their prostate health, as well as how their perceived PCa risk influences this choice. The study’s primary purpose is to gain understanding of the meaning of the lived experience of Jamaican men who have undergone prostate cancer screening.
The research question for the proposed study will be, ‘What is the lived experience of Jamaican men who have undergone prostate cancer screening in the US?’
To attain an understanding of the lived experiences of Jamaican men after undergoing PCa screening, the study cannot adopt standard theoretical foundations of what is already known. New understanding will need a liberal interpretive approach to investigate new realities presently unknown. In social research, a researcher can only assume one of two possible worldviews, when investigating a social reality like PCa screening experiences, namely, objectivistic worldview otherwise known as positivism and the constructivist worldview (Crotty, 1998). Positivistic research assumes the objectivism worldview, where reality is investigated in concrete formal measurements, common in quantitative research (Crotty, 1998).
Constructivist research on the other hand interprets meaning of a social phenomenon, from the subjective point of view of the participants in a specific context. An interpretivist is a social constructivist and thus stands as the opposite of an objective positivist (Munhall, 2007). Interpretivist researchers construct meaning regarding the realities within a unique social context (Creswell & Miller, 2000). Consequently, “constructivists believe in pluralistic, interpretive, open-ended, and contextualized (e.g., sensitive to place and situation) perspectives toward reality” (Creswell & Miller, 2000, p. 125). Interpretivism is thus often referred to as an anti-positivist paradigm (reaction to positivism), or constructivism, where such lived experiences of Jamaican men after PCa screening emerge as alterable realities and not absolutely true to conventional/standardized expectations. Indeed, “constructivism’s relativism assumes multiple, apprehend-able, and sometimes conflicting social realities that are the products of human intellects but that may change as their constructors become more informed and sophisticated” (Guba & Lincoln, 1994, p. 110).
Leitch, Hill, and Harrison (2010) recommended that, interpretivism research is largely not based on a theory but it enables a research to internalize its procedure and process “within the underlying research philosophy rather than something to be tested upon completion” (p. 68). This reality “requires a shift from the notion of validity as an outcome to validation as a process” (p. 67). Black (2006) argued for the critical necessity of relativistic research. Interpretivism is anchored on a word-based description of contextual meaning of phenomena. Black (2006) debated how “words can fully express the meaning inherent in our observations, personal interviews, and pictures when so much of it is subtle, hidden, and contextually bound” (p. 319). After conducting a thematic review of the literature on the interpretivism paradigm, the scholar ultimately credited the paradigm a credible, reliable, restrictively necessary, and essentially comprehensive on precise contexts (Black, 2006).
In agreement, Grix (2004) asserted that, “the interpretive epistemology is one of subjectivism, which is based on real world phenomena,” a social reality, investigating the subjective meanings ascribed to a phenomenon by human actors (p. 83). Subjectivity anchors a research study within social contexts of a specific population, where findings are only relevant to the perceptions and understanding of people in that phenomenon (Cohen, Manion, & Morrison, 2007). Nursing research focuses on the realistic world where participants are active humans (Upadhyay, 2012, p. 123). Nursing researchers must therefore understand what “they see, hear and read from the people and places and from events and activities” and progressively “learn about some aspects of the social world and to generate new understandings that can be used by that social world” in health care programs (Upadhyay, 2012, p. 123). Derivatively, it emerges that investigating the lived experiences of Jamaican men after PCa screening in a manner that attains reliable understanding, requires new meanings to be constructed or interpreted about PCa screening.
Interpretivism frames its legitimacy from the context-dependent meaning generated in phenomenology (Kelliher, 2005). Indeed, according to van Manen (1988), interpretivism establishes the presence of a phenomenon and thus prompts adequate understanding of realities in that phenomenon (phenomenology). In this regard, the lived experiences of Jamaican men after undergoing PCa screening emerge as a unique phenomenon. According to Blaikie (2004), “the study of social phenomena requires an understanding of the social world that people inhabit, which they have already interpreted by the meanings they produce and reproduce as a necessary part of their everyday activities together” (p. 509).
The chosen philosophical template approach can be traced from Crotty’s (1998) presentation of the relationship among theoretical perspectives, methodology, epistemology, and research method. Understanding will only be generated after interpreting lived experiences from the unique context of Jamaican men in the U.S., and constructing meaning thereof, as the research findings. The figure below illustrates the interpretative paradigm to be employed when implemented in this proposed study.
Figure 1. Foster. (2016), The paradigmatic schema, adapted from Crotty, 1998. with modifications I rearranged this figure citation. Please check with your editor to make sure this revision is correct.
The proposed study will implement a qualitative research methodology. To Creswell (2007), qualitative research helps understand people, events, and situations. The proposed study will focus on understanding lived experiences of Jamaican men after undergoing PCa screening. Given that the study will primarily focus on interpreting and constructing meaning, Munhall (2007) commends the qualitative approach as the only feasible empirical process that enables a researcher construct knowledge regarding a phenomenon. The qualitative research methodology was specifically chosen because it answers the “what,” “how,” and “why” questions rather than merely investigating the “how much” and “how many” questions often answered using quantitative research methods (Polit & Beck, 2004).
Qualitative research is based on the utilizes inductive reasoning, where meanings are neither concrete nor objective. Meanings can only be constructed from the perspective of lived experiences of the humans within the context under study (those experiencing the phenomena being researched). The researcher can therefore only employ open-ended, broad methods of primary data collection (mostly interviews), to generate narratives, pictures, and word-based descriptions (the qualitative data)(Creswell, 2007).The qualitative research approach is based on the philosophical underpinnings of post-modernism, where the research deconstructs and reconstructs meaning (Polit & Beck, 2004). Creswell (1998) described qualitative research as an ethnographic and non-experimental study grounded in the lived experiences of participants and purposed to interpret meaning. This description of qualitative research agrees with Berg’s (2007) definition of qualitative studies as the description of “meanings, definitions, characteristics, concepts, metaphors, symbols, and the description of things” (p. 127).
Marshall and Rossman (2006) have argued that qualitative researchers operate under the assumption that a community is structured with logic and order, such that knowledge is contextually determined rather than an objective truth. Consequently, to implement a qualitative study, the researcher must describe the phenomenon under study (PCa screening), based on the lived experiences of the participants (Jamaican men). As such, qualitative researchers need to integrate the information they collect with the description of the context and observation of the participants to develop or construct meaning of lived experiences. The researcher must be immersed within the data collection setting, in an effort to understand the phenomenon under study from the viewpoint of the participant who lives within that setting (Creswell, 2007).
According to Marshall and Rossman (2006), to understand this contextual meaning, the researcher must approach such knowledge from the perspective of the participants who operate within the context under study. The active and interactive engagement of the researcher with the participants is therefore essential to construct meaning from qualitative data (Creswell, 2007. By investigating and exploring the lived experiences of those who determine the knowledge under study inter-subjectively, a researcher can then establish a neutral meaning of the context-specific knowledge. Consequently, the qualitative research approach is most for constructing multiple realities/meanings of a phenomenon, and by doing so, enabling a comprehensive understanding of variant circumstances from the perspective of such participants as Jamaican men (Creswell, 2007).
Typical of naturalistic research that constructively interprets meaning, Creswell (2007) and Munhall (1994) asserted that qualitative research approach seeks the understanding of lived experiences. In the proposed study, the qualitative research approach will help understand how Jamaican men interact with PCa screening sessions and how they make sense or develop meanings based on their lived experiences. Quantitative research seeks to test the relationship of variables with statistical measures, while as qualitative research describes such relationships with rich and in-depth narratives, written words, and pictures, rather than measures the variables statistically. The proposed study needs a qualitative research approach to describe and interpret meanings as understood by the Jamaican men who undergo PCa screening, interpretively and without generalization.
Five philosophical assumptions are foundational to scientific inquiry. These assumptions serves as the scientific lens from which the investigator approaches the investigation. In this qualitative study, research is anchored on the five philosophical assumptions namely: (a) ontological, (b) epistemological, (c) axiological, (d) rhetorical, and (e) methodological assumptions (Creswell, 2007) will be reviewed and discussed from that perspective: As explored below, these assumptions will be relevantly significant to the proposed study.
Ontology Assumption. The ontological assumption proposes that the nature of reality is subjectively constructed to reflect the world, such that, qualitative research focuses on what is known of the world (Creswell, 2009). The proposed study will seek to investigate the lived experiences of Jamaican men, to understand the subjectively constructed meanings evoked by PCa screening.
Epistemology Assumption. The epistemology assumption focuses on the relationship holding between the researcher (knower) and reality (what is known and is being investigated), where a qualitative researcher participates in the study based on the transactional subjectivism foundation. The researcher will participate in the data collection from the position of a Jamaican man in the US, within the high-risk age bracket, and thus sharing identity with the participants.
Axiological Assumption. The axiological assumption holds on the role of values when constructing meaning (van Manen, 1990). In qualitative research, meaning is constructed based on significant influences of researcher and participants’ values, to yield value-based findings. The proposed study will generate findings from the perspective of Jamaican men in the US, based on their own understanding and interpretation of PCa screening procedure, and without imposing any third party perspective. This meaning will be the product of their cultural, social, economic, and political environment, and thus unique from any other meaning generated outside that context.
Rhetorical Assumption. The rhetorical assumption supports the informal and literal language used when conducting qualitative research. To describe the lived experience of Jamaican man after undergoing PCa screening, cannot be described in a formal and statistical language that is otherwise suitable for quantitative studies. The findings will be described in a manner that derives meaning with an in-depth and detail rich language that is widely accepted in qualitative research (van Manen, 1997; Creswell, 2007).
Methodological Assumption. The methodological assumption centers on the inductive research methodology employed in qualitative study (Creswell, 2007). Qualitative research investigates “a topic within its context and continually revise questions based on experience gained,” thus cannot have a predefined and standardized research method (Creswell, 2007, p. 18). van Manen (1990, 1997), concluded that there are no fixed set of research methods for qualitative research, particularly phenomenology. This conclusion accrues from the fact that, “there is no prescription about the unanimous methodological sets of doing a hermeneutic phenomenological research” and can only “suggest for few methodological guidelines” (Kafle, 2011, p. 194). The methodological assumption thus proposes variant of qualitative research methods with “the purposive sampling with information rich cases” (Merriam, 1998, p. 62). Further, for data collection and generation, a qualitative researcher can collect data using interviews, observations, and protocols, to generate “life world stories the research participants, depending on the context and the area of research the appropriate tool can be applied” (Kafle, 2011, p. 194).
Notably, while van Manen (1997) recommended that collected data should be and processed by “uncovering the thematic aspects” (p. 59). Laverty (2003) recommended a data analysis performed by “applying the hermeneutic cycle that constitutes of reading, reflective writing and interpretation in a rigorous fashion” (p. 24). The proposed study will employ thematic analysis of face-to-face interview data and observations, to create meaning after reading, reflecting and interpreting resultant meanings. Only such a process will help conclusively understand the lived experience of Jamaican men in the US, following PCa screening.
Largely a philosophical framework, phenomenology has gradually evolved as a central research mechanism method in health science, and while contemporary phenomenology is the child of such scholars as van Manen (1994), Edmund Husserl and Martin Heidegger originally inspired the research framework.
Husserl and Heidegger are the philosophical fathers of two distinctive meanings and brands of phenomenology – namely interpretive (employed by the present study) and descriptive (Munhall, 2012). Husserl focused on tracing central ground of lived experience when defining the world based on human understanding (Moustakas, 1994). Husserl thus inspired a descriptive brand of phenomenology, where the investigation of a phenomenon can only come from an isolated and objective standpoint. Researchers must therefore investigate phenomena without feelings/bias, “by seeing, clarifying, and determining meaning and by distinguishing meanings” objectively (Munhall, 2012, p. 64). Notably, Husserl focused on epistemology, thus mandating the use of descriptive bracketing to eliminate potential bias. From an epistemological approach, therefore, Husserl conceived the use of descriptive brackets to eliminate biased subjective participation of a researcher in the research process.
Heidegger differed with Husserl’s worldview and introduced interpretive phenomenology, in what became “hermeneutical transformation of phenomenology” (Munhall, 2012, p. 67). To Heidegger, a researcher is human and can thus only interpret the meanings of phenomena by subjectively experiencing and journaling the experiences shaped by the culture, history, values, and worldviews of actual participants, from their perspective (Munhall, 2012). Since individuals can only interpret what they experience subjectively (not objectively), Heidegger defined phenomenology as an accurate reflection of knowledge, awareness, and beliefs shared by people who experience the phenomenon.
Ultimately, Husserl conceived humans as constitutes of states of consciousness while Heidegger countered that consciousness is peripheral to the dominance of an individual’s existence. In comparison, Husserl focused on epistemological use of descriptive bracketing, whereas Heidegger focused on ontology, thus eliminating the need for descriptive bracketing when a researcher subjectively interprets phenomena as a participant in the research process. To Heidegger and subsequent scholars of interpretive phenomenology, researchers are viewed as interrelated with the world, and they can only develop/interpret meanings by active engagement with the participants who experience the phenomenon. Only then can they attribute meaning to their personal consciousness (Munhall, 2012).
As Creswell (2013) observed, such studies rely on “intentionality of consciousness” as a research methodology where a researcher’s consciousness becomes the very basis of giving meaning to a reality (p. 59). Heidegger thus became the father of hermeneutic phenomenology as adopted by the present study. Hermeneutic phenomenology enables a researcher to interpret lived experience of people, and the interpretive process is achieved through a hermeneutic circle, which moves from the parts of lived experiences. This view is different from descriptive phenomenology of Edmund Husserl, who believed in the experience of living or being, not the process of how things are known (Creswell, 2007).
Eventually, after Husserl and Heidegger inspired the philosophical foundation of phenomenology (both interpretive and descriptive), the ground was set for subsequent expansion of phenomenological research. Several researchers have advanced the field in history, but for the present discussion, this inquiry will exclusively focus on Maxvan Manen (1990) who inspired the contemporary brand of phenomenology principles. Rather than adopting either an interpretive or a descriptive approach as inspired by Husserl and Heidegger, van Manen (1990) integrated and overlapped descriptions and interpretation as part of the research process and further added language and lived experiences as part of investigating process of world meanings. Contemporary phenomenology is a systematic approach to expose and explain the composition of the lived experience interpretively (van Manen, 1990).
van Manen’s contemporary phenomenologist was inspired by Heidegger but progressively introduced a lived-experience perspective to the research process and is implemented as a research methodology with two philosophical perspectives – namely; hermeneutics and phenomenology (Creswell, 2007). According to van Manen, (1990), phenomenology is enriched by understanding and meaning from the perspective of both the participants and the researcher, where experiences lived in a phenomenon reveals significant meanings for accurate interpretation and description. Modern scholars concur, notably Creswell (2009), Munhall (1994), and Crotty (1998), that the structured reflection of a people’s consciousness is what defines phenomenology today.
To construct the reality, therefore, the researcher must first interpret individuals’ reflection within the context of the phenomenon under review. From the outset, therefore, the interpretivism approach involved phenomenology, or the study of phenomena as proposed by van Manen (1988), where the focus was to understand the meaning of experiences within a social context. Phenomenology enables researchers to interpret the perceptions of actors/people within the context of a phenomenon, rather than outsiders. In agreement Heron and Reason (1997), argues that, “to experience a world is to participate in it, simultaneously molding and encountering it” (p. 3). Phenomenology today asserts that how people perceive phenomena is based on their experiences from their perspective/consciousness, and interpretivism research assumes this perspective to understand such meanings.
According to van Manen (1994), scientific research needs to interpret a phenomenon with conscious understanding of the human perspectives involved. Indeed, Creswell (2009) defined phenomenology as the study of describing “the meaning of the lived experiences for several individuals about a concept or the phenomenon” (p. 51). As such, “phenomenology is concerned with the study of experience from the perspective of the individual” before such experiences are generalized for the target population in which the individual is a member and actor (Lester, 1999, p. 2). Phenomenology is an esteemed research method, in identifying and establishing “experiences and perceptions of individuals” drawn from their personal perspectives, regardless of the normative assumptions invoked, in a manner that accurately explains a phenomenon in its realistic context (Lester, 1999, p. 2).
Ideally, therefore, the systematic study of a people’s reflection regarding what Husserl (1970) calls “common sense” can be structured as people’s consciousness regarding a phenomenon (Creswell, 2009). Therefore, the proposed study will adopt the phenomenology research design. According to van Manen (1997), phenomenology interprets a phenomenon with conscious understanding of the human perspectives involved. To Creswell (2009), phenomenology is the study of describing “the meaning of the lived experiences for several individuals about a concept or the phenomenon” (p. 51). Edmund Husserl is credited as having inspired the descriptive phenomenology foundations (Crotty, 1998).
Phenomenology is an attempt to construct meaning of a social reality, as a phenomenon. Phenomenology demands that a researcher adopts relativism (rather than positivism), when eliminating “the prevailing understandings of the phenomena,” so that the scientific inquiry is significantly defined by the “immediate experience of the phenomenon,” thus enabling “possibilities for new meanings as an authentication and enhancement of former meaning” (Crotty, 1998, p. 78). A central underlying meaning is defined by a person’s individual experiences within a social context (Husserl, 1970).
In philosophy, phenomenology is concerned with a person’s reality or personal meanings about their “life world” from the perspective of a specific phenomenon (Smith, 2003). Phenomenology as a research approach thus seeks to achieve deeper understanding of the meaning of people’s everyday experiences (van Manen, 1990). People’s awareness and consciousness is subjectively defined in concurrence to the world around them (Munhall, 2007). As such, “distinct subjective and objective worlds do not exist (since) objectivity is only achieved through subjective consciousness or perception” (Munhall, 2007, p. 22). Phenomenology constitutes investigating the meaning of lived experiences, where such meanings are understood in the context of everyday, subjective world (Schwandt, 2001). The four major constructs of phenomenology are: (a) consciousness, (b) embodiment, (c) naturalistic attitude, and (d) experience and perceptions.
Consciousness. Consciousness denotes the awareness of an individual as existing in the world. An individual has a sense of being alive and living in the world, and this awareness is his or her consciousness. When reviewing the phenomenological concept of consciousness, Munhall (1994) quoted Merleau-Ponty (1962) who defined consciousness as the “sensory awareness of and response to the environment” (p. 14). Rather than being a definite measure of what a person feels or thinks (in the interior), or what he or she sees, hears, smells and touches (on the exterior), consciousness focuses on the overall existence of a being (having a body) as part of the world (Munhall, 1994). The study will investigate the consciousness of Jamaican men in the US as a lived experience of being in the world, and after undergoing PCa screening, which is an experience that an individual cannot step out of, given that it is the reality.
Embodiment. Embodiment denotes consciousness or awareness of individuals’ being in the world, their sense of consciousness of the world around them (Munhall, 1994). According to Ellingson (2009), “embodied knowledge is sensory, (and) it highlights smell, touch, and taste as well as more commonly noted sights and sounds” (p. 245). Phenomenology investigates the meaning of reality from the context in which human individuals understand the world, and this meaning is often defined by what the body tastes, sees, feels, hears, thinks and smells(what the body experiences) (Munhall, 1994). Their understanding of the world around them is embodied by their sensual awareness and consciousness.
Conducting phenomenological research involves employing the qualitative research methods that establish the lived meaning as embodied by what individuals within a context, experience/understand about a phenomenon. As argued by Finlay (2009), “phenomenological researchers generally agree that our central concern is to return to embodied, experiential meanings aiming for a fresh, complex, rich description of a phenomenon as it is concretely lived” (p. 6). The qualitative perspective of nursing research seeks to understand a phenomenon based on what Munhall (2007) regards as the realities of a patient’s context. According to Todres (2007), embodiment defines the “touchstones” of phenomenological research, where a researcher inquires about the embodied meaning of a phenomenon as understood/experienced by people within a specific context.
The question of embodiment is essential in nursing research as established by Munhall (2007), and in general health care research as argued by Ellingson (2006). Phenomenology constructs the unique meaning to how people in a particular social situation understand a specific phenomenon (Husserl, 1965). Given that what an individual knows (knowledge) is “grounded in bodily experience encompasses uncertainty and ambiguity” of everyday life, then phenomenology involves “eschewing sanitized detached measurement of discrete variables” that embody an individual’s consciousness within the specific contexts in which they live (Ellingson, 2008, p. 245). Derivatively, phenomenology is thus a study of lived experiences as embodied by their consciousness and awareness of the world around them (Munhall, 1994). Phenomenology thus focuses on the contextual-depth of lived experiences (Cohen, Manion & Morrison, 2007), or the in-depth qualitative knowledge of reality in a social context (Creswell, 2009). As argued by Crotty (1998) phenomenology seeks to understand how individuals’ “consciousness engages with objects which are already pregnant with meaning” (p. 43) for a phenomenon. In the proposed study, the researcher will seek to understand the meaning that Jamaican men in the U.S. ascribe to PCa screening experience, based on their real-life consciousness and awareness.
Naturalistic Attitude. Phenomenology constructs meaning for a reality, in most cases a socially constructed naturally occurring reality (Myers, 1997). Phenomenology adopts a realistic approach when interpreting the awareness and consciousness of a people to construct meaning about what “already is,” the “being,” and what is an abstract “truth” (Husserl, 1982). People understand the world as is, in its natural form, such that any phenomenon is regarded as a natural reality. This contextual meaning is socially constructed, mainly because “the world does not exist independently of our knowledge of it” (Grix, 2004, p. 83). As such, because of the natural attitude, people regard “everything worldly” with an acceptance of being, where existence in the world is a natural truth (Husserl, 1982). As such, phenomenology constructs meaning for “this being-beforehand,” where “the world that is always existent beforehand” and reality emerges from “constant accepted-ness of a basis” as true (Husserl, 1982, quoted in Fink, 1995, p. 166). Phenomenology is thus studying natural meaning that people accord to phenomenon since “a tree is not a tree without someone to call it a tree” (Crotty, 1998, p. 43). The natural process of consciousness and or awareness is bound to change with time and with context variations, as demonstrated in nursing research (Munhall, 2007).
Phenomenology explores the reality a phenomenon, as it already is (Remenyi et al., 1998) and expands the theoretical knowledge available on a phenomenon. According to van Manen (1988), phenomenology helps expand the theoretical knowledge regarding a phenomenon, or to Yin (2003), phenomenology generates meanings of a naturally accruing phenomenon. People in any social context thus approach life with a naturalistic attitude and give a subjective meaning to a phenomenon. Qualitatively ascribing meaning to phenomena is a firm foundation of social research, given that, reality only emerges when human beings encounter consciousness and ascribe meaning to diverse phenomenon (Crotty, 1998). Given that phenomenology is defined by context, individuals, and by subjective meaning attributable to a reality based on the experiences and perceptions of such people (Creswell, 2009; Gephart, 1999; Willis, 1995), the proposed study will seek to understand PCa screening experiences from the perspective of individual Jamaican men in the U.S. context.
Experience and Perceptions. In phenomenology, meaning is derived from the experiences and perceptions that define how people in a specific context understand a phenomenon. As such, phenomenology helps construct subjective meaning of a social phenomenon, based on the experiences and perceptions of a specific population who live in a specific context. Reeves and Hedberg (2003) asserted that the phenomenology “stresses the need to put analysis in context,” since the meaning derived regarding a phenomenon, is subjectively unique to the experiences and perceptions the people give to that phenomenon (p. 32). Derivatively, phenomenology seeks, “to understand how members of a social group, through their participation in social processes, enact their particular realities and endow them with meaning, and to show how these meanings, beliefs, and intentions of the members help to constitute their actions” (Orlikowski & Baroudi, 1991, p. 13).
As soon as people adopt a naturalistic attitude towards a reality in their world and use their embodied experiences of awareness and consciousness to adopt meaning for that context, then reality become the outcome of their experiences and perceptions. Phenomenology seeks “to understand the fundamental nature of the social world at the level of subjective experience” and by so doing, constructs an “explanation within the realm of individual consciousness and subjectivity, within the frame of reference of the participant” (Burrell & Morgan, 2005, p. 28). The subjective experiences and perceptions of individual Jamaican men in the U.S., will thus define the meaning they give to the phenomenon of PCa screening after undergoing the procedure.
A researcher can choose from several approaches when implementing a phenomenological study. The proposed study will adopt a hermeneutic phenomenological approach to interpret lived experiences of individuals in a community. Hermeneutic phenomenology focuses on interpreting people’s lived experience in a natural setting, by describing the meanings accruing from such experiences. To van Manen (1990), a human science needs to combine phenomenology and the hermeneutics approach. Such a study seeks to investigate how everyday human experiences gain specific meanings via human science (van Manen, 1997). Creswell (2007) concurs that phenomenology is the study of describing “the meaning of the lived experiences for several individuals about a concept or the phenomenon” (p. 51). While phenomenology focuses the lived experience from the perspective of a phenomenon, the hermeneutics approach specializes on understanding the phenomenon from the context of humans (van Manen, 1997).
While phenomenology helps “construct an animating, evocative, descriptive of human actions, behaviors, intentions and experiences as we meet them in the life world,” hermeneutics uses human-centered description and interpretation of the lived experiences (van Manen, 1997, p. 19). Conducting phenomenology from a hermeneutic approach optimizes the findings of a research study. According to van Manen (1990), research needs to interpret a phenomenon with conscious understanding of the human perspectives involved. Phenomenology principles integrate hermeneutics to mold a philosophy on experiences of living, rather than on the process of how things are known (Rodgers, 2005). The proposed study will thus investigate the phenomenon of PCa screening and the lived experiences that result from undergoing the screening, from the perspective of Jamaican men. In conclusion therefore, the proposed study will adopt a qualitative research background with a constructivism approach, employing interpretivism perspectives when implementing a phenomenological research study.
Hermeneutic Phenomenology for this Study
Several studies, including Consedine, Adjei, Horton, Joe, Borrell, Ramirez and Neugut (2009), Rivera-Ramos and Buki (2011), Nanton and Dale (2011), Morrison, Aiken and Mayhew (2014), McCree-Hale, Hale, Rutley, Aung and Jolly (2012), Jones (2008), Eldemire-Shearer, Mitchell-Fearon, Laws, Waldron, James & Holder-Nevins (2014), Edelstein and Gillath (2008), Anderson and Marshall-Lucette (2013) have established non-adherence of Jamaican men to PCa screening. These studies have established what is known about Jamaican men and PCa screening, precisely that there are social, cultural, and economic barriers to their PCa screening adherence. What is absent in the contemporary knowledge is the lived experience of Jamaican men after undergoing PCa screening. Understanding this meaning requires that lived experiences are not discovered as concrete standard truths but instead as uniquely constructed realities absent in current knowledge. Since “constructivists, do not assume any single reality and believe that empirical reality and theoretical concepts are mutually constitutive” (Blatter& Blume, 2008, p. 327), the constructivist philosophical background, as the one adopted here, is most suitable for such a study.
This study is inspired by a realization that PCa incidences have reached disastrous levels among Jamaican men, both in prevalence and mortality. As the literature review establishes in Chapter 2 of the dissertation proposal, PCa is treatable if diagnosed early enough. Unfortunately, Jamaican men are dying by the thousands, simply because they are not diagnosed or because they were diagnosed too late, when successful treatment was no longer feasible.
The proposed study will attempt to understand what the arguably controversial procedure means to some Jamaican men who choose to undergo PCa screening when they are still asymptomatic and healthy. Most importantly, researchers have previously identified cultural influences and biases as the major deterrents for Jamaican men to undergoing PCa screening. The proposed study will seek to understand how healthy Jamaican men resolve or reframe these negative forces. By understanding the meaning and interplay of the knowledge, attitudes, and beliefs that healthy Jamaican men ascribe to PCa screening, the study may identify specific resources and possible interventions for the entire group of Jamaican men currently facing the health disparity and optimize their adherence to the critical nursing intervention.
It is hoped that The findings generated by the proposed study may serve the best interests of all healthcare stakeholders in the U.S. who pursue PCa screening-aided benefits among high-risk communities. These stakeholders incorporate all Jamaican men in South Florida and beyond, healthcare professionals (notably nurses), hospitals and clinics, health insurance firms, and the government.
Nurses have a social contract to protect and promote individual and public health and well-being. A major responsibility of this relationship is to identify and ameliorate health disparities. Men of color and Jamaican men, in particular, face clear health disparities in prostate cancer morbidity and mortality and in PCa screening (Eldemire-Shearer et al., 2014). The ethical, professional, and social duty of nurses is to employ the best possible strategies to improve the health status of any community, particularly if facing disparate morbidity and mortality rates from a condition that can be successfully treated if diagnosed early. According to Davies (2011), modern “nurses are well placed to encourage and support patients to make healthy choices” (p. 20). It is therefore essential that nursing researchers and scholars investigate this issue as an urgent and significant health problem.
An empirical investigation of the choice to undergo PCa screening by adherent Jamaican men may reliably help identify context-specific motivations to improve standard PCA screening practices towards optimized effectiveness. Researching the meaning and importance that healthy Jamaican men ascribe to PCa screening may help to inform nurses in understanding what motivates positive health seeking and preventative behaviors in this at-risk population (Kelly et al., 2011). Based on this knowledge, nurses may be better positioned to identify and advocate for health policies to reallocate resources and to redesign educational materials that may not only facilitate adherence to PCa screening but may also decrease the health disparities in PCa and PCa screening that disproportionately impact Jamaican men. The results of this inquiry may not only advance nursing knowledge, it may also advance the science of nursing.
Contemporary nurses are being educated, like their pioneer trainees, are learning how, why and when to implement PCa screening as standard nursing intervention. This however has failed to increase the adherence to such vital screenings, and the standard anti-PCa campaigns have been ineffective for the Jamaican group of immigrants. Without question, therefore, nursing education needs to go beyond a standard care approach and cater for diverse contextual, cultural, and socio-economic patient profiles to improve the health outcomes of communities that have previously been secluded and unequally considered.
As such, future nursing education needs to incorporate “essential transcultural nursing concepts, principles, practices, and policies” that adequately prepare future nurses to offer optimal health care for a multi-cultural globe (Leininger, 2002a, p. 8). Ideally, the findings generated by the proposed study might inspire modern nursing education to accommodate a new era of fighting PCa with effective strategies for diverse contexts. The proposed study may help identify specific resources and possible interventions for such a population as Jamaican immigrants, who often ignore and deliberately avoid an essential nursing intervention, based on the understanding the meaning and interplay of knowledge, attitudes, and beliefs held by the healthy Jamaican men who adhere to such an intervention.
The effectiveness of a practicing nurse is not merely on doing what is possible, what a patient wants, or what should be done for any patient in a specific clinical procedure. Nursing involves active participation of the professional nurse, to recruit and motivate the commitment and cooperation/support of a patient when exercising positive health behavior. Nursing practice thus needs to acknowledge the contextual differences of patients, and refine their approach in a manner that best serves the health interest of such patients. Consequently, the study readily acknowledges the need to optimize effectiveness of community healthcare programs, particularly those aimed at providing PCa screening to American immigrants.
As previous studies have affirmed, an element of cultural, social, health knowledge and event economic significantly influences and defines the adherence of Jamaican men to PCa screening. This is what the nurse must know, understand, and refine to approach the non-adherent community based on the insights generated from the healthy men who do attend PCa screening. Only then, will the nurses be able to deliver optimal PCa screening programs to the Jamaican men, with positive health outcomes. The proposed study was primarily designed to inform this gap in knowledge and generate findings that will be invaluable to community and clinical nurses within the U.S.
From the perspective of practicing nurses, therefore, the findings generated by the study is hoped to be invaluable to practicing nurses, not only those facilitating PCa screening for Jamaican men but also every professional nurse offering community health in diverse contexts. Contemporary health and public policy often provide a collective and generalized health program for all citizens in a country. Some communities negatively receive standard health care programs due to their lived experiences. Cultural, economic, and social ideologies of immigrant communities, for instance, mold some living experiences that require more than standard community health programs. Health programs and policy needs new anti-PCa programs that strategically provide for the unique experiences of Jamaican immigrants. The findings may inform nurses working in health care facilities on the best way to attend to diverse contexts and to optimize PCa screening outcomes. Practicing nurses may be informed by the findings generated by the study, to understand how a community’s lived experience following PCa screening mandates the use of variant nursing approaches for optimal health outcomes.
According to Powers and Knapp (1995), nursing research was designed to develop knowledge about issues of importance to nurses in a way that enables practicing nurses to describe the characteristics of a particular nursing situation about which little is known. Nursing research aims at explaining a phenomenon that must be considered in planning nursing care, predicting the possible outcomes of certain nursing decisions, controlling the occurrence of undesired outcomes, and initiating activities that may promote desired health behavior as argued by Polit and Beck (2001). Indeed, as Polit and Beck (2001) concurred, advancement of nursing research enables the acquisition of knowledge necessary for the nurse to practice competently and design efficacious interventions based on scientific data, to improve patient care continually.
It is therefore notable that previous research has failed to review outcomes of PCa screening for such a community as Jamaican men. Almost all research findings generated in the last two decades, regarding the high-risk population of Jamaican men, and their non-adherence to PCa screening, has exclusively focused on those who avoid screening. The questions have ranged from why Jamaican men avoid PCa screening, to how they can be informed and encouraged to undergo the screening. Previous nursing research has only focused on one side of the phenomena and never considered those who do attend such screenings. In truth, therefore, previous research on PCa screening and Jamaican men has therefore been piecemeal inadequately informing.
Consequently, the findings generated by the proposed study may help redefine nursing research to be more comprehensive. Communities need more than just the scientific merit of PC screening when fighting worsening PCa mortality. There is urgent need for accurate research findings on what happens during and after PCa screening. Besides the traditional approach to nursing practice, modern nursing needs to extend into the concept of caring, where patients become more than recipients of health care services, but human beings who need a nurse’s personal involvement (Leininger, 1969).
The study may provide a new approach to nursing research, captivating a novel understanding of the context in which PCa screening is delivered, among unique patients. Beyond recommending the benefits of PCa screening, the proposed study may embrace the need for the diverse patient care for optimal PCa screening outcomes. Most notably, the study will be based on the lived experiences of the patients who devotedly opt to seek for such interventions despite coming from a community that prefers to avoid screening as a health care intervention.
When a government invests increased resources to improve the health status of a community, focusing on the provision of resources and manpower to enable a community prevent, manage and control such a disastrous diseases, as a PCa, chances of success are improved. This has been norm of community health policy in the U.S. and particularly among the otherwise marginalized immigrant communities. Arguably, Jamaican men in South Florida have higher opportunities of fighting the PCa disaster that has previously threatened their health than any other ethnic and racial group. The number of facilities available, manpower committed to the PCa screening programs, and the reduced cost of undergoing the procedure, is evidently very hospitable than it is in many other areas across the globe.
These advantages, however, are meaningless to a community that devotedly and intentionally avoids such screening, for whatever reason – cultural, social, or economic. Regardless of how much is invested and planned, any health care policy that does not attain desired outcomes is misinformed, as are most PCa screening policies for immigrant populations in the U.S. These screening policies need to be updated and modified. An empirical investigation of the choice to undergo PCa screening by adherent Jamaican men may reliably help identify context-specific motivations to improve standard PCa screening practices towards optimized effectiveness. Researching the meaning and importance that healthy Jamaican men ascribe to PCa screening may help to inform nurses in understanding what motivates positive health seeking and preventative behaviors in this at-risk population and revise contemporary health policy appropriately (Kelly, Melnyk, Jacobson & O’Haver, 2011). Based on this knowledge, advocacy for health policies can seek for the reallocation of resources and the redesign educational materials to not only facilitate adherence to PCa screening but also decrease the health disparities in PCa and PCa screening that disproportionately affect Jamaican men.
The proposed research study will consist of a purposeful sampling of men presently residing in South Florida, who have Jamaican origin but are now immigrants to the U.S., and who have already undergone PCa screening. The proposed research participants will incorporate English speakers aged above 40 years, who have already participated in a single PCa screening procedure in a standard health care setting. The study will be conducted within the jurisdiction of South Florida, where the population of Jamaican men is highest within the U.S., and based on strategic convenience of the researcher.
The foregoing scope of the study will predefine the potential limitations of the study. The sample will be recruited using purposive sampling, anchored on convenience and reference. Not only will the age bracket of respondents make the PCa screening overly sensitive, but also the timings for interview sessions will have to be sensitive to the age bracket. Many of the respondents will predictably speak the Jamaican dialect of English, rather than Standard English, which will limit communication when recorded and quoted for the dissertation. Further, upon recruitment, the researcher will collect data using broad and open interviews, where the open-ended questions posed to the participants will be highly reliant on their understanding and interpretation. In agreement with van Manen (1997), the researcher will actively participate in the interviews so that during the interaction, the lived participants may be understood based on their meanings within an accurate context (Polit & Beck, 2004). Nonetheless, the potential limitations have been accepted as central to phenomenological nursing research, and the findings will be qualitatively comprehensive and reliably accurate (van Manen, 1997).
This chapter discussed the background of the proposed study and introduced the area of interest under research. The chapter thus justified the proposed research undertaking on PCa risks, from the perspective of the global, Caribbean, and American PCa risk factors of Jamaican men. Based on the background, the chapter developed a literature-based statement of the problem shaping the study’s purpose, broad aim, narrow objectives, and research questions, on understanding the lived experiences of Jamaican men in the U.S. after undergoing PCa screening. The chapter also critically reviewed the philosophical underpinnings upon which the study is anchored (qualitative research methodology, interpretivism paradigm, phenomenology research, and hermeneutic phenomenology research design). Finally, the chapter briefly reviewed the significance of the proposed research findings to nursing, nursing education, nursing practice, nursing research, and public health policy, before highlighting the scope and limitations of the proposed study.
The proposed study will seek to understand the lived experience of Jamaican men who have undergone the screening procedure. Important to note, the foregoing first chapter only gave brief coverage to the area of interest for the present study. This chapter was developed to serve this goal with a systematic review of relevant literature.The review evaluates what scholars and practitioners have established regarding PCa, PCa screening, PCa screening experiences, and Jamaican men.
All the other literature review sources used will be identified, selected, traced, and accessed online. The researcher will employ a set of key words and phrases to implement the search process, online. The Google Search Engine will be used to trace the most relevant and feasible sources. Notably however, most of the key words and phrases identified in academic research databases will be employed. The key words and phrases to be used will include (a) prostate cancer, (b) prostate cancer screening, (c) Jamaican men and prostate cancer, (d) Jamaican men and prostate cancer screening, and (e) PCa screening experiences.
Using the list of key words and phrases identified above, the researcher will then have to identify the most reliable academic databases in which the key words were used to locate literature sources. The databases were consulted to trace the most relevant and reliable literature sources, had to purely provide academic content, feature a listing of the most advanced and popular academic journals, and have a reliable search mechanism. The key words and phrases will therefore be used as tools to search in academic databases, such that relevant articles selected and traced on the topic of interest, and the quality and outcomes of such a search will be influenced by the databases in which the search is conducted. Most notably, the databases to be selected for use will include (a) PUBMED, (b) Centers for Disease Control (CDC), (c) Cumulative Index to Nursing and Allied Health Literature (CINHAL) Plus, and (d) Ovid E-Books.
Once the key words and phrases are entered into the database search engines, it is expected that hundreds of articles will be identified as search results. The next step will then be selecting the best, relevant, reliable, and most credible literature sources from the search results. An inclusion/exclusion criterion will be used, specifically developed to determine which literature sources provide the most reliable, accurate and comprehensive knowledge to be incorporated in the systematic literature review.
The criterion will be (a) the literature sources either reported an empirical research study (primary research) or discussed the PCa screening and Jamaican men, (b) the literature source must have been published between 2010 and 2015, and (c) the literature sources must be a peer-reviewed academic publication. Further, (d) the literature source must have all the appropriate features of a high quality academic publication, and (e) the journal article article must have several or any one of several of the following topics, namely Prostate cancer screening, Jamaican men and prostate cancer, Jamaican men and prostate cancer screening, as well as PCa screening experiences.
All articles in the search results that do not meet the criterion listed above will be excluded from review. Notably however, although all the selected articles must have been published within the last five years, several selected articles will be selected although they were published beyond the five-year limit. These specially selected sources will primarily be characterized as being valuable seminal works and their findings were very significant and critical for the present study, on the topic of interest. Most importantly however, the foregoing search process has already been implemented and yielded satisfactory results. Only the articles that meet the foregoing criterion were be selected for the review, as such, the following content areas will be presented … although the process will also be repeated and expanded when preparing the final dissertation report. You need to list the content areas as they appear in the review starting with historical context
The literature provides a convincing argument on why it is critically important to investigate the experiences of Jamaican men after PCa screening, to determining whether such screening attain the objective and purpose that the PCa screening movements was geared at attaining from their onset. After selection, the literature sources were then subjected to a critical review, systematically implemented to serve the interests of the proposed study. To begin the review, the present section will trace the historical background of PCa screening, focusing of the conceptual threads of PCa screening experiences for Jamaican men, and integrating the disciplinary perspective of nursing into the review. In the sections that follow, the historical review will discuss the PCa risks levels in the globe, in the Caribbean, in Jamaica, and in the U.S. followed by linking Jamaican Men in U.S. and PCa risks, and finally profiling PCa screening as an intervention measure in contemporary health care.
Globally, PCa has emerged as one of the most sensitive type of cancers based on the number of incidences and mortalities recorded annually. In the second edition published at end of 2015, Djavan, Bostanci and Kazzazi (2015) addressed the “epidemiology, screening, pathology, and pathogenesis” of PCa. According to the authors, PCa is now the leading type of cancer among men, both in the incidence and mortality rate, particularly among the black and Caribbean populations. According to Sinfield, Baker, Agarwal, and Tarrant (2008), PCa patients recorded the worst experiences compared to the experiences recorded with other type of cancers including breast and stomach cancers.
In 2012, Center, Jemal, Lortet-Tieulent, Ward, Ferlay, Brawley and Bray (2012) reviewed the “international variation in prostate cancer incidence and mortality rates,” and noted an increasing global incidences (largely in developed nations), and mortalities (in less developed nations) (p. 1079). Importantly for this study however, Center et al. (2012) reported that, “estimated PCa incidence rates remain most elevated in the highest resource counties worldwide including North America, Oceania, and western and northern Europe” (p. 1079). Above the question of economic development, there emerged a notable trend about where most incidences and mortalities were recorded. Indeed, when reviewing global statistics of PCa incidences, there is also a unique bias for a specific racial profile.
Centers for Disease Control and Prevention (2015) reported a PCa deaths/mortality trend defined by both race and ethnicity. Between 1999 and 2012, CDC reported that “the rate of men dying from prostate cancer has varied, depending on their race and ethnicity,” where Caribbean and black/African men are “more likely to die of prostate cancer than any other group, followed by white, Hispanic, American Indian/Alaska Native, and Asian/Pacific Islander men” (p. 2). Confirming this trend, the International Agency for Research on Cancer, on behalf of the World Health Organization reported that in 2012, the world registered over 14,068,000 new cases of cancer (incidences), formally diagnosed and triggering the deaths of 4,653 000 men (Globocan, 2015). According to the report, over 15, 296, 000 men had died of cancer between 2007 and 2012 (Globocan, 2015).
From a global point of view, the Caribbean region alone triggers the highest number of incidences every year, compared to any other region (Prostate Cancer Caribbean, 2008). Based on PCa incidence, prevalence, and mortality rates recorded in the Caribbean nations by 2008, showed that Caribbean men alongside African men recorded the highest recorded risk of developing PCa cancer. The genetic makeup of black and Caribbean men triggered a risk value higher than that of any other racial profile (Glover, Coffey, Douglas, Cadogan, Russell, Tulloch & Walsh, 1998). Consequently, Gibson, Hanchard, and Waugh (2010) reported that black and Caribbean populations have the highest risk of developing PCa in the world.
In the Caribbean region, cancer incidences registered nationally in Jamaica, the Bahamas, Cuba, Trinidad and Tobago, Grenada, and in Martinique have qualified the Caribbean as one of the most high-risk locales of PCa (Prostate Cancer Caribbean, 2008). Aiken and Eldemire-Shearer (2012) reported that, of greater concern in the rising PCa incidences statistics globally, is the indication “that the Caribbean region has the highest age-standardized PCa-specific mortality rate in the world at 26.3/100 000/year” (p. 90). Confirming on the global and Caribbean incidence rates, a unique PCa trait becomes evident, from the perspective of the Jamaican nation. PCa is now most common among black populations in the world, among whom Jamaica is perhaps the most predominant representative of nations with the highest rate of PCa incidences (Gibson, Hanchard & Waugh, 2010; Glover et al., 1998). Aiken and Eldemire-Shearer (2012), findings confirmed that Jamaica represents the Caribbean nation with the highest rates of PCa. According to Gibson, Hanchard, and Waugh (2010), based on incidences reported between 2003 and 2007, PCa is “the leading cancer affecting men in Jamaica (p. 456).
Traditionally, “the highest reported incidence of prostate cancer in the world was thought to be among United States black men,” and never did any study focus on the Caribbean immigrants (Glover et al., 1998). Eventually, statistics showed that the incidence rate in Jamaican capital, Kingston alone, reached 304/100,000 men, 80% of whom were pathologically confirmed. A higher risk value was subsequently identified among Jamaicans in Jamaica, that in African men, with 30% of the patients having “acute urinary retention, 16% presented with bone metastases, 15% with gross hematuria at the time of diagnosis and 42% with an abnormal rectal examination suspicious for cancer” (p. 1984). Most importantly, Prostate Specific Antigen (PSA) was measured among Jamaican sat only 7% of the PCa cases in 1989 reached “48% of cases by 1994” (p. 1984).
Morrison, Aiken, and Mayhew (2014) reported that in Jamaica today, PCa “accounts for almost a third of all cancers diagnosed” with Jamaica having “the highest incidence of PCa in the world, based on a reported rate of 304/100,000 per year” (p. 456). According to records by the Jamaica Cancer Registry, PCa “is the most common cancer overall as well as the most common cancer in men” with an “age-standardized incidence rate of 78.1/100,000 per year” (p. 456). Even more concerning is that, by 2014, PCa was “the most common cause of male cancer-related deaths, with an age-standardized mortality rate of 53.9/100,000 per year” (Morrison, Aiken, & Mayhew, 2014, p. 456).
It is also apparent that the high risk of developing PCa affects not only Jamaicans within Jamaica, but also those who have immigrated to the U.S. According to Kendrick (2010), “research has shown that prostate cancer is the second leading cause of cancer death among men in the United States and Caribbean and African American men are more likely to develop the disease than White American males” (p. 6). Jamaican men residing in the U.S. thus depict a similar high PCa risk as those in Jamaica.
The American Cancer Society (2008) and Gibson, Hanchard and Waugh (2010) established that Jamaican men have the highest rates of PCa even within the U.S., when profiles by race and ethnicity as Caribbean. In their study, Gibson, Hanchard, and Waugh (2010) reviewed all cancer cases recorded in Jamaica’s biggest cities (St. Andrew and Kingston) which totaled to 4981 cases, among which 2536 were among males between 2003 and 2007. For men, the “age standardized rates per 100,000 per year” stood at 188.8, with the leading type of cancer being PCa.
Glover et al. (1998) conducted an epidemiology of PCa in Jamaica, whose population are majority of African descent, and compared their statistics with those “of white and black Americans” (p. 1984). To conduct the study, the researchers profiled 1,121 PCa diagnoses between 1989 and 1994, sourcing the information from the government pathology laboratory, Jamaican Cancer Registry, clinic and hospital records, as well as physician office records, and ultimately computing the incidence rates with the 1991 national census in Jamaica. Following the study, Glover et al. (1998) confirmed that Jamaican men “have a high incidence of prostate cancer, much higher than even black Americans during a similar period,” notably with PCa showing “more significant clinically with greater morbidity in Jamaica than in the United States” (p. 1984). The American Cancer Society (2015) affirmed that, based on global cancer fact and figures, PCa cancer incidences and mortalities are higher in the U.S. than in the Africa and the Caribbean, yet within the U.S., the highest rates are among the Caribbean (notably Jamaican) and African men.
PCa screening denotes a procedure, done to investigate presence of cancerous cells in the prostrate, and is “used to discover clinically significant disease early in the disease process to prevent mortality and morbidity through treatment” (Aiken & Eldemire-Shearer, 2012, p. 90). Similar “high risk” screening approaches are when conducting mammography to diagnose breast cancer, the antenatal screening alongside faecal blood used to diagnose colon cancer, or papanicolau smears used to diagnose cervical cancer (p. 90). Focusing on Jamaica as the core of the Caribbean territories with the highest rates of PCa, Aiken and Eldemire-Shearer (2012) argue that the early disease stages of PCa are often asymptomatic and cannot be linked to, or help signify the development of the condition.
Without symptomatic indications of the onset of PCa, the condition easily develops from its onset to the mature stages without detection (Bowen, Hannon, Harris, & Martin, 2011). Consequently, prostate cancer screening has to date become the most reliable, accurate and sustainable method of diagnosing PCa in its early treatable stages. In their study, Aiken, and Eldemire-Shearer (2012) examined the role and significance of PCa screening among the Jamaican population, where PCa conditions are mostly “identified after symptoms appear” as established by Aiken, Tulloch, Freeman, Bennett, Coard, Panton and Flanigan (2003), and identified when the condition has already matured to fatal stages (p. 90).
Screening has been advocated for to determine the population of cancerous masses in several types of external cancer, as well as used in some high-risk diagnostic procedures for internal cancer (Aiken & Eldemire-Shearer, 2012). There has been significant debate for and against the use of screening to test and diagnose PCa. As such, PCa screening has become one of the most reliable strategies “to decrease the risk of death from this disease (p. 725). However, sections of the literature have highlighted the mismatch of screening results and clinical interventions that follow. According to these scholars, PCa screening faces “a significant risk of over-detection and over-treatment of tumors that would not have caused morbidity or death” (Aiken & Eldemire-Shearer, 2012, p. 91). Even the slightest cancer masses detected after a PCa screening can therefore trigger PCa treatment that is an exaggeration of idea preventative and treatment measures, when such patients would have survived without concerns, even if the PCa screening were never conducted.
The debate on the suitability of PCa screening has incorporated the concerns of medical practitioner, interests groups in the medical community, policy makers, community health stakeholders, and the public. Prime among these concerns is “the question of whether prostate cancer screening achieves its stated objective of reducing prostate cancer-specific mortality whilst minimizing the potential for harm amongst screened individuals” (Aiken & Eldemire-Shearer, 2012, p. 91). Previous research has integrated a myriad of variables and case-specific determinants, including ages, time spent during and after screening, length of detection, reliance on volunteer candidates (96% of whom are healthy and without PCa), demographic features, and number of years a PCa patient lives after screening in contrast to potential number of years without PCa screening. The variables helps determine whether PCa screening improves the life of screened patients, reduces the severity of development, and helps patients survive fatal outcomes.
Today, the core essence of screening is in enabling timely and reliable diagnosis of PCa. Haas, Delongchamps, Brawley, Wang and De la Roza, (2009) observed that, “prostate cancer is the most frequently diagnosed non-skin cancer in the United States and the third leading cause of cancer deaths,” yet the only validated means of intervening against PCa mortality, is often disregarded. Haas et al. (2009) reviewed studies published in the International Agency for Research on Cancer, Surveillance, Epidemiology National Cancer Institute databases, and established that, “prostate cancer incidence is dependent on efforts to detect the disease,” and that when used, PCa screening “provide accurate and useful information regarding comparative prevalence rates of the disease among regions of interest” (p. 3866).
The proposed study will exclusively focus on a specific population of Jamaican men, currently residing in the US. Jamaican men originated from the Commonwealth nation of Jamaica, still a monarch of England under the rule with of Queen Elizabeth II, and an administrating head of state. Among all Caribbean islands, Jamaica is the third largest with an assortment of mountainous typography bordering a lengthy but narrow coastal plain (Sherlock & Bennett, 1998). The capital city of Jamaica is Kingston, which is the largest of urban areas in the country alongside such cities Ocho Rios, Mandeville, Port Antonio, and Montego Bay (BBC, 2015).
With a censured total population of 2.7 million based on United Nations profile (UN, 2011), Jamaica is dominantly occupied by Black population with an African ancestry (BBC, 2015). Indeed, the Black population represents 92.1% of the population, in contrast to other ethnic profiles including Asian at merely 0.8% of the population. An outcome of the slave trade triangle, Jamaica was a porting site for slaves arriving to the U.S. from West Africa, which explains the close political and social link between Jamaica, Britain, and the U.S. (Mullally, 2003). Indeed, according to Richardson, Tibbles, and Schwarz (2007) the dominant black population in Jamaica are either “of African or partially African descent,” most of whom “trace their origins to West Africa” (p. 41).
However, while most identify themselves as black, they have mixed ancestry commonly denoted as Anglophone Caribbean (Richardson, Tibbles & Schwarz, 2007). Within and without Jamaica, the people have their major and official language being English (official), although majority of the citizens speak English dialect Patois (Jones, 2008). Majorities are dominantly of the Christian religion, and the life expectancy of Jamaican men is 71 years, slightly below the 76-year life expectancy of Jamaican women (BBC, 2015). Jamaicans have migrated with an overwhelming number to the U.S., Europe and of recent, Asia. As such, “more than half of migrants absent from Jamaica in 2007 went to the United States, while around 15 percent went to the United Kingdom,” according to Glennie and Chappell (2010, p. 3).
As such, while most Jamaicans presently reside in the U.S. and England, can only be credited to the slavery roots of their ancestors (Sherlock & Bennett, 1998), new generations of Jamaicans have also immigrated to seek for education and employment outside the Caribbean island (Mullally, 2003; Glennie & Chappell, 2010). The Jamaican in the U.S. are referred to as Jamaican Americans, who according to are American citizens of either partial or full Jamaican ancestry, with a distinctive cultural identity (Jones, 2008). Today, the most Jamaicans reside in the New York City, South Florida, Philadelphia, New Jersey, Tampa, Boston, and Atlanta. State-wise, the 2010 national census recorded 965,355 American residents of Jamaican origin, the largest Jamaican populations being in (i) New York (305,285), (ii) Florida (246,478), and (ii) New Jersey (55,351) (Glennie & Chappell, 2010). Above that, among the communities with highest percentage of Jamaican residents is Miami, Florida, with over 6.3% of Jamaican adults (Jones, 2008).
PCa screening has been linked to distinctively significant experiences among Jamaican men. A section of the literature suggests that, Jamaican men approach, regard, and respond to PCa screening based on their awareness and knowledge of PCa and PCa risks. In the paragraphs that follow, the paper first reports, reviews and critically synthesis several recent studies on the most essential fields of knowledge relevant to the proposed study, as highlighted by the sectional headings for each are of review.
McCree-Hale, Hale, Rutley, Aung and Jolly (2012) conducted an experimental survey to “evaluate the impact of a theory-based health education intervention on awareness of prostate cancer” and the resultant intention to undergo screening among Jamaican men (p. 580). To implement the study, the researchers sampled 188 Jamaican men who attended outpatient clinics. Data were collected using pre and post-test interviews and surveys, both before and after “a health education intervention” on PCa and PCa risks (p. 580). In the study, McCree-Hale at al. (2012) purposed to evaluate the impact of a theory-based health education intervention on awareness of PCa and intention to screen among men in Jamaica.
Ultimately, the researchers found that, health education on PCa significant increases the acceptance, adherence, and consistence of PCa screening decisions among aware and informed Jamaican men. Indicatively therefore, based on McCree-Hale et al. (2012) findings, most Jamaican men would avoid, ignore and fail to undergo PCa screening for lack of awareness and knowledge on their risk of developing PCa and the role of PCa screening. McCree-Hale et al. (2012) asserted that, “theory-based patient education can promote awareness of prostate cancer and informed screening methods including potential risk associated with screening behaviors” (p. 580).
A quantitative survey conducted by Bowen et al. (2011). The quantitative survey investigated the decision making of Jamaican men and attending PCa screening. Bowen et al. (2011) conducted the survey across the Washington state, randomly sampling men above 50 years in age. Data was also collected from “a simple random sample of primary care physicians, were conducted in the same geographic area,” focusing on PCa screening rates and practices among men, either through PSA or DRE, among the practicing physicians (p. 155). The findings revealed that, while PCa screening was commended by all sampled physicians, Bowen et al. (2011) found that provision of relevant information enabled “increasing informed decision making about prostate cancer screening” (p. 155). The link between informed decision making among all men besides Jamaican men, adequately aware about PCa, and attendance to PCa screening was also affirmatively generated by Bowen et al. (2011) in their empirical study.
Consedine et al. (2015) conducted a systematic review of PCa trends among Caribbean migrants to the US, both of African descent and Caribbean natives. From the 15 research articles previously published, Consedine et al. (2015) reviewed PCA tendencies among the men. Ultimately, they study concluded that “Caribbean men of African descent screen less frequently than is recommended” (p. 915). As such, whether already adequately informed or otherwise, whether PCa screening facilities are accessible, and the procedure affordable, Jamaican men perceive PCa screening based on their lived experiences. It is of great concern that some Jamaican men subscribe to “misperceptions about cancer risk,” where PCa is regarded as “a taboo topic,” excluded from discussion or consideration by virtue in cultural beliefs and social norms (p. 209).
Another related study was conducted by Consedine, Tuck, Ragin, and Spencer (2009) in the US. Consedine et al. (2009) They used a stratified cluster sampling method to recruit 5333 from four distinctive ethnic groups namely, (a) Jamaican immigrants, (b) African Americans, (c) European-American, and (d) immigrants from Trinidad and Tobago. In the study’s implementation, The researchers synthesized three previous empirical studies that they had conducted on the fear/loathing of PCa screening among Caribbean ethnic sub-populations in Brooklyn, New York. While using a systematic literature review, the study exclusively reviewed three empirical studies that had been conducted by the same scholars in the same jurisdiction with the same purpose. As it emerged, The data revealed that even among Jamaican men in the US, screening is regarded emotively, such that the decision to screen or not is the outcome of emotional patterns of thought (Consedine et al. 2009). The fear of PCa, fear of undergoing the screening procedure, overwhelming anxiety, and emasculation concerns among immigrant Caribbean men in Brooklyn, New York, influence their perception of and adherence to PCa screening (Consedine et al. 2009).
Several other empirical studies have recently contextualized the PCa screening adherence rates. The first study was conducted by Anderson and Marshall-Lucette (2013). Employing a qualitative research design, Anderson and Marshall-Lucette (2013) using a purposive sampling method, the study recruited 214 African and Afro-Caribbean men at a hospital in the UK, and then employed face-to-face interviews. Following the in-depth interviews, the researchers conducted thematic analysis of the primary data with the purpose of gaining “an insight from these men’s perspectives and ascertain whether a more focused health promotion strategy, and specific UK-based research, was needed” concerning PCa careening (p. 1296). In its outcomes/results, the qualitative study The data generated four main themes of “disease-prompted awareness, checking up as a necessary evil, defining and constructing factors influencing prostate cancer screening uptake, and appraising perceived myths about prostate cancer through personal beliefs” (p. 1296).
Notably, Marshall-Lucette (2013) established that the socioeconomic status of men in the community, such as education and professional background, were factors that influence their level of awareness of PCa and prompted their decisions to seek help. Further, according to the study, the men’s perspectives that a more specific health education strategy that promotes early detection and management, targeting African and Afro-Caribbean men, would help in demystifying PCa and encourage them to seek help earlier. Similar findings as those generated by Marshall-Lucette (2013) were reported nearly a decade earlier in the US.
Evans et al. (2005) conducted an empirical study that informs shapes, inspires, and justifies affirmatively, the research study proposed herein, and like the present study, the researchers investigated the impact of demographic, racial, cultural and gender features to the adherence and non-adherence of a target population to PCa screening alongside breast cancer. The study provided a contextualized understanding of the concept of adherence and non-adherence as employed in the proposed study, this instance focusing on the target population of Jamaican males currently residing in Broward. Evans et al. (2005) employed a participatory-action research method when collecting data from focus groups, on two occasions/phases. The sampled participants were five African Nova Scotian men and women, sampled from a population of 57 individuals who were already validated as free from or diagnosed as having either prostate cancer and breast cancer. Ultimately, Evans et al. (2005) established that there is a significant link between culture and gender (particularly of femininity and masculinity perceptions) among the African Nova Scotian community in Canada.
This influential background “unavoidably interact with other social structures such as race and class to affect women and men’s perceptions and experiences of these two cancers” (p. 257). Consequently, Evans et al. (2005) validated the need to consider the meanings and implications that social, cultural and demographic features impose on such critical health interventions as PCa screening and breast cancer tests. In their words, it is mandatory for “health care professionals to have an understanding of the overlapping and contextualized nature of gender, class, and race and be willing and able to work in partnership with African Nova Scotian communities to identify and develop strategies that reflect the realities of peoples’ lives” (p. 257).
Key among the argument used when supporting, recommending and qualifying PCa screening is the prospect of conducting PCa screening at almost any demographic context, easily, with a standard procedure, at an affordable cost, and regularly. Significantly important for the present study proposal is that, adherence of Jamaican men to PCa screening invokes a consideration of their lived experiences, and by so doing invokes an influence of their Jamaican culture. Evans et al. (2005) researched how cultured relations influenced African Nova Scotians to attend breast and prostate cancer tests in Canada, as part of their lived experiences and resultant perceptions. Further, while the study proposed herein will focus on the male gender when investigating non-adherence of Jamaicans to PCa screening, Evans et al. (2005) provided a broader research parameter by investigating gendered relations (male and female), that differently influence breast and prostate cancer tests among the African Nova Scotians. From the study, Evans et al. (2005) found that the act of seeking health care services, particularly those focused on reproduction health, is perceived by men to being weak, vulnerable and feminine.
A decade later, Clarke, Soler-Vila, Fleming, Christ, Lee and Arheart (2012) thematically analyzed data from National Health Interview Survey, alongside a detailed document analysis in the US, to compare screening trends and adherence among all cancer survivors, working survivors, and the general population since 2000. After recruiting 174,393 participants, the researchers quantitatively “compared the screening trends among all cancer survivors, working survivors, and the general population over the last decade” followed by a thematic analysis of the results (p. 190). During the analysis, the investigators observed a decrease in PCa diagnosis in the U.S. beginning the year 2000, accompanied by an increase in the number of recorded cancer survivors after successful treatment. According to the scholars, “cancer screening behaviors among survivors may play an important role” in the diagnosis and treatment process of cancer, particularly the early detection of such cancers as prostate cancer, since the “screening protocol increases early detection of secondary tumors and reduces potentially limiting side-effects” (p. 190).
However, for diagnosis and treatment, the concept of adherence is a critical mark after initial diagnosis, including during the post-treatment stages of cancer. It also appears that PCa screening only increases when men understand their risk factors of developing PCa. On the overall therefore, the study thus affirmed that, “healthy people goals as a measure of desired adherence” principle helps underscore the need for consistent, reliable, and best-practice health behavior when fighting such a disease as fatal as PCa (Clarke et al., 2012, p. 190).
Perhaps this argument justifies the research findings generated by Roumier et al. (2004) at the start of the century. Roumier et al. (2004) They conducted an experimental study to assess “the adherence to an annual PSA screening program” in a period of 3 years, as well as identify the “characteristics of men who failed to undergo the full screening process” (p. 280). The 442 sampled men had a first-degree relative diagnosed with PCa, and participated in an “annual serum PSA testing over a 3-year period,” and data was collected using questionnaires (p. 280). The study found that participants without genetic PCa susceptibility recorded high levels of non-adherence, but those with close relatives already diagnosed with PCa had an 88% adherence rate. Notably, therefore, having a close relative diagnosed with PCa (genetic susceptibility) increases the adherence of an individual to screening.
Finally, for the present discussion, Rivera-Ramos and Buki (2011) conducted a qualitative hermeneutic phenomenological research design study to “examine cultural and gender beliefs and how these influence Latino men’s attitudes, beliefs, and behaviors related to prostate cancer screening” (p. 13). From a purposive sample of 10 Latino men, aged 40 and above years, who were not linked to PCa, and or had attended any PCa screening. In this study, the researchers conducted a structured survey alongside face-to-face interviews. The analyzed data established that (a) all participants valued the manly image of ‘Machismo,’ which overruled the need for PCa screening, (b) misconceived screening procedures as having healthcare professionals “insert a finger!” and (c) the perception of manliness defied seeking healthcare assistance with sexuality-related issues, thus influencing their PCa screening non-adherence.
Steadley, I am not sure what the problem is but this section is not well organized, sometime you report the studies correctly, sometimes not! This section should be organized as follows: After indicating, the content areas that you will address then report the historical studies systematically. Once you have completed that then repor on the identified content area. Each content are should have as abare minimum three studies up to about 5 studies. For each study you MUST report, aothot, year, study type, purpose, sample size, data analysis method, results. At the conclusion of the content area, you need to do your synthesis in which you compare and contrast the reported studies and then conclude with the purpose of your study and what your study will cover. I know this is a tedious section but you cannot short cut or short change!!!
The proposed study captures an extremely sensitive area of interest for the researcher. Being a practicing nurse, the researcher in the jurisdiction of the study, South Florida, will explore the best possible interventions that can help protect a community that is not only in danger, but also one he feels obligated to serve. It is therefore important to mention that the researcher is a Jamaican by birth, before immigrating to the U.S. for further education and to pursue a professional career. The Jamaican community in the U.S., and globally at large, has recorded immense economic, political, and social progress in the last few decades. This progress is owed to exceptional athletes, committed politicians, highly trained economic experts, advanced scholars and numerous other Jamaican nationals who positively contribute to the community in assorted ways and from hundreds of separate fields.
The present researcher thus acknowledges, with appreciation, the need to contribute to the community in his area of training and expertise, namely nursing. As the country progresses in health care provision, within and without Jamaica, the highest numbers of men who die because of PCa are Jamaicans. As noted severally in the foregoing sections, this is similarly true among Jamaicans who reside in the world’s sole superpower. It is an obligation and a professional commitment, that the researcher explores ways to avert this trend and participate in improving the quality of life for a people with whom they share and identity. Such knowledge would be critically important not only for Jamaicans, in the U.S. and elsewhere, but for many other communities facing the aggressive impact of PCa.
The foregoing testimony captivates the professional and personal perspective of the researcher, which will significantly influence how the findings are interpreted and narrated. The researcher is, in all ways, focused on determining the accurate and reliable empirical meaning that Jamaican men attribute to PCa screening. It is hoped that such findings will help optimize the role of screening, among a high-risk population, and thus prevent unnecessary deaths that can and should be avoided. van Manen (1997) commends and recommends that researchers should investigate a phenomenon they feel connected to, yet one in which they avoid being too intimate with in a manner that determines the knowledge attained.
Nonetheless, the researcher will at risk of collecting and analyzing the primary data with significant risks even with all the foregoing strategic steps. This fear is real for the researcher, and a cause of concern. Reviewing qualitative research studies among health professionals, Jeanfreau and Jack (2010) concurs with the researcher, observing that, “many practicing health educators do not feel fully confident in their ability” to conduct qualitative studies (p. 612). Indeed, Jeanfreau and Jack (2010) cites several previous studies and scholarly books, most notably Porter (1993), Jootun, McGhee, and Marland (2009), who all contend that, “qualitative researchers acknowledge that there is a possibility that their values and beliefs may influence their research studies” (p. 612).
With this fear therefore, the present researcher will employ strategic bracketing of the data, and precisely accommodate reflection as part of the data collection process. According to Jeanfreau and Jack (2010), bracketing denotes how a researcher acknowledges “the possible influence and an intentional setting aside of conscious thoughts and decisions influenced by the particular mindset” while reflexivity denotes a “researcher’s self-awareness and the strategies the researcher used to manage potentially biasing factors while maintaining sensitivity to the data” (p. 612). In agreement with Porter (1993), and Speziale and Carpenter (2007), Jeanfreau and Jack (2010) recommend that, any “possible effect of the researcher’s influence can be reduced through bracketing and reflexivity,” where a researcher’s core responsibility in qualitative is anchored on being “self-aware of one’s own reactions, reflections, and even personal growth along with the researcher and participant relationship” (p. 612).
The present scholar will adopt Chan, Fung and Chien’s (2013) qualification of bracketing. According to the scholars, the use of bracketing helps demonstrate “validity after initiating a phenomenological study” particularly in “the data collection and analysis process” regarding a phenomenon (p. 1). Based on the commendation, bracketing the data will initiated not only during the actual data collection and during analysis process, but also now as the researcher prepares for the study. According to Chan, Fung and Chien’s (2013), “the concept of bracketing should be adopted upon initiating the research proposal and not merely in the data collection and analysis process,” (p. 1) to ensure that the researcher does not negatively influence or invalidate the planned study.
The present researcher therefore appreciates that the shared background may influence how the values, experiences, feelings, and assumptions expressed by the participants are interpreted. The influence however, will help make the meanings clearer and accurate, but not to inhibit how such experiences and feelings are interpreted using bracketing. As van Manen (1990) argues, phenomenology requires the researcher to participate actively, in investigating the reality, and thus knowledge emerges as a co-creation of both the researcher and the participants. As such, being a Jamaican man within the age bracket of the participants will be vital in co-creating knowledge when implementing the study, since the researcher will better understand the participant’s perspective, identify with it, and interpret it precisely and accurately.
Further, graduate training and professional experience of the researcher, will help anchor the study from the perspective of nursing, and only incorporate personal involvement as a reflection of the data collection process. PCa screening will be reviewed and investigated as a nursing intervention in the control of PCa. The researcher will understand the participants from the perspective of a practicing nurse, when they explain their experiences during and after screening. As such, the study will better capture the meaning of such narrated experiences, with the additional nursing edge, than would be possible without the nursing perspective.
It is also important to note that the study will be best served by a phenomenological research design, than by any other comparative design. To exemplify, the appropriateness of phenomenology for the area of interest, two previous studies attained critically essential knowledge simply because they were phenomenological. The proposed study can best be served by a phenomenological approach, just as the same approach was ideal for Rivera-Ramos and Buki (2011), as reviewed in a foregoing section. As such, the knowledge generated by Rivera-Ramos and Buki (2011) about the phenomenon of PCa screening among Jamaican amen, could only be described qualitatively, and not quantitatively or otherwise.
Similarly, Friedman et al. (2009) focused on “cancer information-seeking behaviors, capacity to use information, and recommendations for messages and message delivery” among the sampled participants. Therefrom, Friedman et al. (2009, p. 204) identified the major barriers to effective PCa communication with African-American men to include fear of PCa, cultural bias for privacy of matters related to sexuality, sex and reproductive health, poor resources to enable community health intervention, limited family communication, and negative social perception of reproductive health.
What Friedman et al. (2009) revealed was a complex phenomenon of privacy/individualized, economic, social, cultural, and community health influences to how an immigrant community that has perhaps the highest risk of infection, and whose approach to the fatal condition, is questionable. Optimizing communication with this target population even within the South Carolina context required an integration of the economic, social, cultural, and community health factors that influenced their understanding and perception of PCa. It is predictable that these men would also face similar barriers, when deciding on PCa screening, and most probably, they would not adhere to such PC screening sessions. This derived assumption however, was given credence by the empirical findings generated by Kendrick (2010).
Kendrick (2010) employed a phenomenological interpretive research design among a purposive sample of 11 African American men, to investigate “the relationship of erectile dysfunction relative to prostate cancer screening among African American men” (p. 7). The participants were aged 35 years and above, all of whom were college-educated, with a middle-class social status, and residing in the California Metropolitan region of Greater Sacramento. Following the study’s implementation, Kendrick (2010) established that, “African American men avoid prostate cancer screening due to the perception that a positive diagnosis and treatment may impact sexual relations” (p. 6). Importantly, this reality is what shapes the approach that African American men takes when PCa conditions trigger erectile dysfunction, and even worse, any erectile dysfunction that is not related to PCa conditions. Among these immigrant communities, attending a PCa screening is perceived as a man’s response to erectile dysfunction (Kendrick, 2010).
None of these two studies would have attained as important findings, were they not based on phenomenology. Similarly, the present study will seek to investigate a phenomenon of undergoing PCa screening, which is best based on a qualitative description and interpretation of what the Jamaican men feel, think, and understand. As such, the study will largely rely on the subjective understanding, perceptions, and experiences of the Jamaican male population, and mandates a hermeneutic phenomenological research design from a nursing perspective.
This second chapter provided a comprehensive and critical review of the most reliable knowledge on PCa, PCa screening, PCa screening experiences, and Jamaican men. After described ing the literature search strategy used to assemble the sources used, The chapter provided a historical context of PCa screening, reviewing PCa risks in the globe, in the Caribbean, in Jamaica, and the U.S., highlighting PCa risks for Jamaican Men in the U.S., and qualifying PCa screening as an intervention measure. This was then followed by a review of the research content, providing a geographical and social profile of Jamaica men as the population under study, reviewing previous research on PCa screening among Jamaican men, and sampling previous research on the experience, adherence, and impact of PCa screening. The chapter then terminated with the experiential context, focusing on the researcher’s experimental background, involvement, experience and interests, the use of reflexivity and bracketing, and justifying the appropriateness of the phenomenological research design used. The next chapter will now discuss the research methodology and methods, to be used when implementing the study to investigate the forested gap in contemporary knowledge.
The purpose of the proposed phenomenological study is to explore the lived experience of Jamaican men residing in the U.S., after undergoing PCa screening. This will help the study investigate the meaning that Jamaican men ascribe to undergoing PCa screening as a phenomenon, based on their lived experiences, and thereafter construct a new understanding of how they perceive, think of, and regard PCa screening based on self-constructed meanings. The proposed method will focus on providing a detailed and comprehensive explanation of the research strategies design to be used when conducting the proposed study. The research strategies were selected and planned in an attempt to formulate accurate, reliable, and adequate answers to the study’s research question.
The proposed study will implement a qualitative research methodology to describe the meaning of lived experiences of Jamaican men in the U.S., qualitatively. Creswell (2007) argues that qualitative research is designed to help understand people, events, and situations, based on their lived experiences. The qualitative research methodology was specifically chosen because it answers the ‘what’, ‘how’ and ‘why’ questions rather than merely investigating the ‘how much’ and ‘how many’ questions often answered using quantitative research methods (Polit & Beck, 2004). Ideally, rather than measure quantitatively, the proposed study will focus on understanding lived experiences of Jamaican men after undergoing PCa screening.
Given that the study will primarily focus on interpreting and constructing meaning, Munhall (2004) commends the qualitative approach as the only feasible empirical process that enables a researcher to construct knowledge regarding a phenomenon. Based on Creswell (2007) and Munhall’s (1994) arguments, then the qualitative research approach will help understand how Jamaican men experience PCa screening and how they develop meanings based on their experiences. Quantitative research seeks to test the relationship of variables with statistical measures, while as qualitative research describes such relationships with rich and in-depth narratives and written words, rather than measuring the variables statistically.
Qualitative research helps construct multiple realities of a phenomenon and enabling a comprehensive understanding of variant circumstances from the perspective of participants (i.e. Jamaican men) (Creswell, 2007). The qualitative approach is suitable for constructing multiple realities/meanings of a phenomenon (Creswell, 2007). The proposed study will focus on attaining an understanding of PCa screening experiences, as narrated and described by Jamaican men, to construct meaning of these lives experiences. No other research methodology can serve this purpose as reliably and accurately, above a qualitative research methodology.
Selecting an effective research design as a guideline for the implementation process was now the next important step of the research process. As stated previously, the proposed study will employ a phenomenological research design. Given the onset, history, and progressive improvement of phenomenology as the most reliable and appropriate design in nursing research, the approach was determined as the most fitting to the proposed study. Besides adopting a qualitative research approach, the proposed study will also adopt a hermeneutic phenomenology approach, since the meanings constructed will be based on how humans (Jamaican men), perceive PCa screening. As presented in a diagrammatic illustration here after, the proposed study will employ the six activities constituting the hermeneutic research design as proposed by van Manen (1990), which includes; Identifying the phenomenon of Interest, exploring the phenomenon under study, conduction a reflection on the phenomenology of interest, initiating phenomenological writing process with interpretive narrative and qualitative descriptions of lived experience meanings, implementing pedagogical relation in reporting the study and maintaining absolute research balance when preparing the report.
This phenomenological investigation of PCa screening will focus exclusively on the lived experiences of Jamaican men in the U.S. van Manen (1990) defined phenomenology as an empirical attempt to establish the deep understanding a target group of people hold regarding the nature of their experiences with a phenomenon. To van Manen (1990), argued that a human science study about a phenomenon needs to combine phenomenology and the hermeneutics, to adopt the human perspective. Creswell (2007) and Munhall (1994) qualify the qualitative approach as ideal when investigating the descriptive trait of peoples’ experiences. Munhall (1994) further commends the use of a phenomenological study to investigate experiences and occurrences of a phenomenon.
Creswell (2009) described phenomenology as a study to determine the deep meaning that people’s experiences ascribe to that phenomenon. This reality introduces the element of people as participants to be studied with a phenomenon, using a research design and philosophy is referred to as hermeneutic phenomenology (Munhall, 1994). According to van Manen (1994), scientific research needs to interpret a phenomenon with conscious understanding of the human perspectives involved.
Creswell (2009) defined phenomenology as the study of describing “the meaning of the lived experiences for several individuals about a concept or the phenomenon,” thus integrating the need to include people when constructing meanings of a phenomenon (p. 51). van Manen (1990) best explains phenomenology as an empirical attempt to establish the deep understanding a target group of people hold regarding the meaning of their lived experiences with a phenomenon (i.e., PCa screening). Investigating the lived experiences of Jamaican men after undergoing PCa screening will require the constructivist phenomenology approach, as advocated by Munhall (1994), Creswell (2009), van Manen (1990), and Crotty (1998).
The proposed study will adopt a hermeneutic phenomenological design. Hermeneutic phenomenology focuses on interpreting people’s lived experience in a natural setting by describing the meanings accruing from such experiences. Phenomenology principles integrate hermeneutics to mold a philosophy on experiences of living, rather than on the process of how things are known (Rodgers, 2005). To van Manen (1990), a human science needs to combine phenomenology and the hermeneutics approach to investigate how everyday human experiences gain specific meanings via human science (van Manen, 1997). Creswell (2007) concurs that phenomenology describes “the meaning of the lived experiences for several individuals about a concept or phenomenon” (p. 51).
While phenomenology investigates lived experience from the perspective of a phenomenon, hermeneutics investigates the understanding of a phenomenon from the context of humans (van Manen, 1997). Phenomenology helps “construct an animating, evocative, descriptive of human actions, behaviors, intentions and experiences as we meet them in the life world,” but hermeneutics uses human-centered description and interpretation of the lived experiences (van Manen, 1997, p. 19). Conducting phenomenology from a hermeneutic approach optimizes the findings of a research study, since research needs to interpret a phenomenon with conscious understanding of the human actors involved (van Manen, 1990).
The proposed study will thus investigate the phenomenon of PCa screening and the lived experiences that result from undergoing the screening from the perspective of Jamaican men. By adopting an interpretative hermeneutic phenomenology research design, the study will contextualize the lived experiences (hermeneutic) witnessed by the target population (Jamaican men) and accruing from a PCa screening encounter (phenomenon). Qualitative research primarily focuses on “the interpretation of social world especially of cultures and people’s life-ways rather than seeking causal explanations for cultural practices”(Upadhyay, 2012, p. 123), making interpretivism essential for the study. Consequently, the hermeneutic phenomenology approach will help the interpretative study investigate the meaning, lived experiences, and implications of the case study phenomenon (PCa screening) to the Jamaican men who have already undergone what that the community often avoids.
The figure below was designed as a customized diagrammatic representation of the hermeneutic research design proposed by van Manen (1990), customized to highlight the interests of the proposed study when investigating the lived experiences of Jamaican men in the U.S., after undergoing the PCa screening phenomenon.
Figure 2: The Hermeneutic Research Design and Component Activities (Foster, S. 2016, adapted from van Manen, 1990 with modifications)
The study’s population and setting are directly derivable from the study’s title and area of interest. The proposed qualitative research study will target the Jamaican immigrant community who presently reside in South Florida, U.S. Since the study is solely concerned with PCa screening, the population will be further limited to the males. The study will target the population of male Jamaicans, aged between 40 and 75 years, the age bracket with the highest PCa risk, and who have already undergone PCa screening.
Given that the proposed study will exclusively target the population of male Jamaican immigrants to the U.S., who currently reside within the South Florida jurisdiction, the sampling procedure will employ a purposive procedure, strategically executed to select the most appropriate participants. Towards this end, the researcher has developed the inclusion and exclusion criteria to be used to ensure that the sample recruitment process is conducted with accuracy and precision for the right participants.
Inclusion Criteria. The inclusion criteria was developed objectively for the empirical study, such that the study can be replicated without undue bias, and the study’s participants can be reproduced using similar inclusion decisions. As such, the study will only recruit individuals to be respondents/participants if they qualify through a precise inclusion criteria. The inclusion criteria will consist of Jamaican male immigrant to the U.S., fluent when communicating in American English, currently residing in South Florida, born in Jamaica, aged between 40 and 70 years of age, and self-identify as having undergone PCa screening. Recruited participants will either married or single, with any type sexuality, parents or otherwise, and in low, middle or high income brackets, since these traits are not significant to the interest of the study.
Exclusion Criteria. When selecting participants for the face-to-face interviews, candidates will be excluded from the sample if, they are not Jamaican immigrants to the U.S., not within the 40 and 75 years age bracket, are not male, self-identify as having not undergone PCa screening, and if unable to communicate in standard American English.
Qualitative research mandates a sampling strategy that allows a narrow sample range, where sampled participant meet a predetermined criterion of importance (Patton, 2002). Consequently, the proposed studies will employ a purposive sampling procedure, strategically executed to select the most appropriate participants. Ideally, the study will use a snowball sampling procedure to recruit participants in the qualitative research process. Snowball sampling provides the most appropriate sampling method for allowing a researcher strategically select sources of information-rich data (Creswell, 2007; Patton, 2002).
In the proposed study, the snowball sampling procedure will ensure that selected participants have already undergone the phenomenon of PCa screening, an attributes essentially critical to nature of the study (Patton, 2002). The researcher will seek permission to access barbershops, churches and community centers where Jamaican men congregate from the person in charge of the respective setting. After documented permission to access the prospective participants is received, the researcher will place a flyer announcing the study same message in the approved accessed location, and then discretely and personally meet with any volunteer, inform them about the study, its purpose, and their potential role. Selection of participants will be guided by the inclusion/exclusion criteria. listed above, to select initial interviewees, and even when recruiting participants. Finally, absolute anonymity will be granted to all men who agree to participate in the study, with or without their request, a feature that will be used to encourage participants not to fear discoloring their identity when discussing such a culturally sensitive issue as PCa. Participants will be invited to select a pseudonym in an effort to maintain confidentiality. If the participant is not able to or does not wish to identify a pseudonym then one will be assigned.
Qualitative research is not mandated to attain generalizability of findings, although it is mandated to attain a representation of the target sample (Crotty, 2004). As such, qualitative studies are not obligated to recruit a sample size proportional to the target population (generalizable), above attaining a reliable degree of representation (Creswell, 2009). According to Creswell (2007), the ideal sample size for a phenomenological study should range between 5 and 25 participants. As such, sample selection for the proposed study will include a maximum of 20 participants or until saturation is reached.be based on a progressive search of saturation as recommended by Munhall (2007), Denzin, and Lincoln (2003), to a maximum of 20 participants.
The proposed study will be conducted in accordance to with all standard ethics standards mandated in any scholarly researchcriteria. The ethical considerations to be observed have been described and signed in the IRB form, alongside complementary documents attached as appendices to the dissertation proposal. Among the ethical considerations and standards to be observed, will be the optimal protection of the participants as human subjects. While the researcher will participate in the reflection of lived experiences after PCa screening, the reflection will assume a non-personalized approach when posing questions to respondents. The researcher will ensure that all participants are treated with respect and dignity, and that they are addressed with social decorum and privacy. The researcher will provide adequate time for respondents to respond to questions and discuss the phenomena, while collecting the data. The participants will face no significant risks or harms in their participation.
The study will only involve participant who are able to express consent. Even without compulsion to participate, participants will be informed about the study and its purpose, before being requested to participate voluntarily. The research purpose, objective, and research question will be provided and explained to all respondents during recruitment and in preparation for the data collection process. This guarantee will not only ensure that they are adequately informed/aware of what is required of their participation, but to ensure that their participation is based on an informed decision. All participants will only be involved after signing consent form.
The proposed primary data collection process will require the recruitment and participation of human subjects from South Florida. It is expected that one of the biggest barriers the researcher will face when recruiting participants for the study, will be the unwillingness of the men to discuss such a culturally sensitive topic as PCa, with a stranger. This will potentially delimit the recruitment of participants. The researcher acknowledges that the respondents will predictably be uneasy when addressing PCa. Consequently, recruitment will be voluntary and without coercion. All participants will be approached and recruited with absolute confidentiality. It will also be important to consider their image, respect, and dignity in all ways during the data collection process. Personal identity used to recruit participants will be held in absolute confidence. As such, since the study will be addressing a culturally and socially sensitive subject of reproductive health, with men as old as 70 years, the researcher will assertively assure all respondents that their participation will be held with confidentiality, and with optimal privacy.
The proposed study will employ focus groups and face-to-face interviews, although nearly the entire data collection process will rely on the interviews and the focus groups will only be complementary to the data collection process. The focus groups will only be facilitated after all interviews have been conducted, incorporating a few interviewees, and only to conform the findings generated by the interviews.
Based on the foregoing explanation therefore, the data collection process will largely rely on conducting the interviews progressively. In this respect, the proposed study will adopt the approach commended by Creswell (1998), where the entire process is envisioned in component phases interconnected to form a circle, while conducting the interviews. According to Creswell (1998), data collection involves “engaging in activities that not only include but go beyond collecting data” (p. 117). The personal involvement of the researcher will determine the progress of data collection, since as van Manen (1990) recommends, personal experience of the researcher should be used to shape the data collection process. When participants are selected, informed, and recruited of their participation, they will have signed their consent form and reviewed the ethical template.
The next step will be arranging one interview followed by a second interview session, 90-minute in total, and hosted at social places most convenient to the participants (in place and time). The researcher will identify areas of interest for the study not addressed by the first interview, whose findings are inadequate or inspiring new areas of interest. The goal of each interview will be to collect “good information to answer emerging research questions” (Creswell, 1998, p. 118). These areas will then be addressed by the subsequent interview, progressively, until the research data reaches saturation, and no further areas of research are required (Munhall, 2007). Interviews will be conducted with a guiding schedule, but conducted and maintained in the best possible manner, being cordial and mutually communicative.
The data collection will similarly primarily involve conducting the face-to-face interviews. Upon approval from Barry University IRB to conduct the study, the researcher will place the fliers seeking to recruit participants. It is hoped that the researcher will recruit at least 30 names of Jamaican men who have undergone PCa screening. From the list of 30 potential respondents contacted in absolute confidence, the researcher will select the first 20 who agree to participate. A brief on the research purpose, the ethical template, and the participant’s consent form will be sent to the selected candidates. The potential respondents will be required to have read and understood the documents prior to the first introductory meeting with the researcher.
After the first meeting during which the researcher will respond to any inquiry or question from the potential respondents, the participants will be requested to sign and hand in their consent forms. Only the informed respondents who sign the consent form will be recruited. After recruitment, each respondent will fill a short demographic questionnaire. Ultimately, upon recruitment, the researcher will progressively conduct interviews, each respondent at a time, for between one and three interviews sessions, until data saturation is attained.
When interviewing each respondent, the researcher will use an interview schedule and take brief field notes. The researcher will note both the verbal responses and non-verbal behavior and observe how each participant appears during the interview to capture not only what is said, but also what is indicated by emotions, feelings, and attitudes. The researcher will listen actively, engage in in-depth reflection, follow intuition, maintain cordial conversation tone, and always seek clarification where necessary. The interview sessions will be audiotaped using a (a) cell phone, (b) tablet and (c) laptop, and the best audio copy from the three equipments will then be selected for transcription. At the conclusion of interviews with each respondent, each participant will receive a $25 gift card as a token of appreciation for participating. The researcher will maintain contact with participants, seeking for further information, via phone and email messages. The data will be collected, processed, and stored throughout the process with absolute privacy.
The face-to-face interviews will be purposed to collect data from the recruited Jamaican men, on their lived experiences after undergoing PCa screening. Phenomenological interview searches for depth to discover the everyday lived world of the research participant. The interview will explore meaningful themes in participant specific expression with meaningful description. The themes will however be not pre-defined, but emergent from the primary data collected during the interviews, towards attaining data saturation. The interview will begin with the explanation of the study’s purpose with the research participant by the researcher.
The researcher will ask open-ended question (Appendix…) to elicit an exploration of their lived experience. The response to the questions will enable the researcher to gain an understanding of what it is like for a Jamaican man in the U.S. to have undergone PCa screening. These broad questions will be customized to follow up on each interview progress include, why did you attend the PCa screening, was it your first session or several sessions you have undergone, how old were you when you realized or heard about the need for PCa screening for Jamaican men, and why did you attend the screening session. A list of these questions has been attached as an appendix to the present proposal.
It is also important to note that the study will collect some critically essential demographic data (Appendix…) from the participants. Consequently, the study will use specially designed questionnaire to be filled by all participants prior to the actual interviews, where each participant will provide their demographic profile to accompany the primary data collected during the interviews. The demographic data will assist the researcher understand the situational context better, regarding the phenomenon from the perspective of each participant, and to identifying any commonalities in the data as well as accurately describe the findings based on the profile of the research participant. The specific demographic information to be collected will include nationality (both origins and residence), ethnicity, age of the participants, educational background, profession or occupation, marital status and number of PCa screenings sessions ever attended.
After collecting the primary data, the researcher will analyze the collected data in a manner that responds to research question and research purpose to attain progressive saturation after the first interview. Most importantly, the data analysis process will follow van Manen’s (1990) guidance on analyzing data following a phenomenological study. In the implementation therefore, following the completion of interviews with each respondent, the researcher will select the best possible audio file among the three recorded during each session and complete the audio file transcription. All the audio files for each respondent will be combined into a single transcript file. After receiving transcribed interview scripts, the researcher will edit them to include commentaries and reviews of the content, to integrate the field notes taken during the interviews. The researcher will also review the demographic data for each interviewee from the demographic questionnaire, and combine the data with the edited interview transcript. The demographic data alongside field notes will be used to enrich the meanings of the interview data.
Thereafter, the transcribed files will be analyzed thematically and categorized on how the respondent addresses the selected themes. The data analysis process will thus explicitly align the thematic analysis method, and resultant findings will be dependent on the qualitative themes emerging from the primary data, categorized, narrated, and described to respond to the study’s research question. The process will require that the transcripts be read repetitively by the researcher. Munhall (2007) argued that qualitative data analysis involves examining and arranging data in precise themes, with the goal of gaining an understanding of the researched phenomena.
Further, since the thematic analysis of initial interviews will help refine questions posed in subsequent interviews, to best addresses the themes under analysis, the analysis process will be progressive and improving during the data collection process. Finally, during the data analysis, the researcher will identify how participants duplicate, differ, concur, or broaden the data until a point of data saturation. After the thematic analysis, the researcher will then describe, classify and create a summative interpretation of themes accruing from the data, to generate the findings. Derivatively, the researcher will employ reflexivity to look back on the data collected, relate it to each respondent, contextualize the data with the field notes, and actively participate in the overall analytic process of the themes to construct their respective meanings. Ultimately, the researcher will focus on answering the research question in the most accurate, reliable, and comprehensive manner, based on the collected primary data.
To conclude the third chapter of the proposal, it is also important to review how the researcher will observe the obligatory criteria for research rigor during the study’s implementation. Scholarly and scientific research must necessarily ascribe to the standards of quality that imbue them with trustworthiness and evaluated validity, as reflected by standards of credibility, dependability, confirmability, and transferability (Lincoln & Guba, 1985). As such, in its implementation, the researcher will adopt the standard tradition of qualitative data analysis, in pursuit of attaining optimal rigor in terms of credibility, dependability, confirmability, and transferability of the research findings generated, as reviewed below.
According to Lincoln and Guba (1985), credibility of qualitative research findings refers to the confidence level attained by the data collection process, and the resultant analysis and interpretation, to be true. Research findings gain credibility if they can be believed, and when the entire research process can be understood throughout, as likely to generate credible results for the readers and scholars to and for whom the new knowledge is advanced.
Munhall (2007) alongside Denzin and Lincoln (2003) qualify credibility of qualitative research studies and findings if the quality of the data generated adequately reflect the true human experience being studied. As such, according to Munhall (2007), credible phenomenology necessarily attains the confidence level with believability, if the data generated and interpreted depicts the true reflections of the human actors under review. In the proposed study, the researcher will ensure that the entire study is conducted in a manner whose trustworthiness is credible, validated, and confirmed.
All the primary data analyzed will have originated from the participants, documented with accuracy, and rerecorded in exactness with accurate interpretations from the perspective of the participants. As such, the findings generated will represent accurate and trustworthy interpretations of the primary data collected, absent of the bias and participation of the researcher. The role of the researcher prior to, during, and after the data collection is not to influence the interpretations derivable from the interviews, but to facilitate through active interactions, the participants to provide adequate, comprehensive, and truthful reflections of their experiences.
Dependability of qualitative research findings represents the stability of the data collected and analyzed, independents of contextual elements of time, place and circumstances (Lincoln & Guba, 1985). In the proposed study, the researcher will documents the entire research process, so that future researchers as well as the assigned supervisors can follow through the research process and concur with the same interpretations and conclusions the researcher makes about the experiences of Jamaican men following PCa screening. If future researchers seek to reconstruct the research process, every action will be viable and backed by adequate research evidence to generate similar findings and conclusions.
As such, the researcher will maintain an accurate audit trail, such that the research process will be accurately documented rather than abstract, when generating dependable findings and conclusions. From the sampling procedure, selection of sample, data collection, and data analysis, the study will be resolutely dependable if evaluated, regardless of the time and environmental factors in which the study is conducted. It is hoped that the final report will incorporate a broad and adequately descriptive research procedure for data collection and analysis, and that the report will be based on accurate and comprehensive data. These strategies will be taken to ensure that a similar approach can be used in future, and that future research can affirm and support the findings generated.
Denzin and Lincoln (2003) qualify qualitative findings as confirmable, only is they attain objectivity and or neutrality in the manner the data was collected and analyzed. To Munhall (2007), phenomenological research ought to employ bracketing and objective reflectivity when deriving the interpretations, in a manner that guarantees that similar findings and conclusions can be confirmed for the phenomenon under study. Munhall (2007) recommends the use of journaling in a manner that all data can be authenticated, and where researchers’ opinions, feelings, and subjective experiences do not delimit the objective research process.
In the proposed study, the primary data collected during the interviews will also be complemented by a compilation of field note in the journal, such that the data analysis is not just what the participants said, but also what will not be expressed or communicated non-verbally. The resultant interpretation therefore, will be open to confirmation by parties outside the research process (third parties). The transcribed files will thus include descriptions of feelings, reactions and reflective judgments, all based on the perspectives of the participants and not of the researcher. Importantly, as argued by Creswell (1998) and Crotty (2004), perhaps the most important element of qualitative data analysis to attain research trustworthiness is using member check and confirmation.
Consequently, the researcher will employ focus groups as the second and complimentary data collection instrument. After all the interviews gave been conducted, and the data analyzed, the researcher will then facilitate a focus group. The need to attain credibility, dependability, and confirmability of the findings will also require the concurrence of the participants. The participants will also be given a copy of their transcript alongside the thematic analysis of the interview. Further, the research interpretation of meanings presented as the study’s findings will be read to the participants, seeking for their feedback, conformation, and corrections for any misinterpretation and misinformation, as well additional commentary, on the meanings as interpreted.
Long after the proposed study has been concluded among Jamaican men in South Florida, the researcher hopes that the scientific research process and the findings generated are transferable to similar contexts. While qualitative findings rarely attains the the generalizability of quantitative research findings, qualitative research findings should attain transferability to similar contexts (in settings and sample) besides the locale of the study (Creswell, 1998; Munhall, 2007). To attain this quality of findings, the researcher will document and logically describe the research process in a manner that future researchers can implement a similar study outside South Florida, with another set of sampled participants, and generate similar findings.
As such, the research process from data collection to analysis, will only be employed if it is the most appropriate and feasible for the study, and when bracketing attains credible findings whose conclusions can validly to fill the current gap in knowledge. This will be sensitively crucial in the data analysis stage of the study, where the thematic analysis will be tuned in a manner that is detailed, comprehensive and can be collaborated. In the proposed study, the researcher will implement the thematic data analysis using thematic bracketing, where the data will be categorized ‘as it is’ without bias or subjective influence of the findings generated. Ideally, the researcher will focus on enhance the believability, trustworthiness, and credibility of all findings generated from the study, to ensure that the findings are transferable to other contexts with similar phenomenological constraints.
This third chapter of the dissertation proposal provided a comprehensive explanation of the research strategies to be used when conducting the proposed study. The research strategies were selected and planned in an attempt to formulate accurate, reliable, and adequate answers to the study’s research question. In conclusion, therefore, a hermeneutic phenomenology research design will be used targeting the Jamaicans in South Florida. The study will employ a snowball sampling procedure to recruit between 15 and 30 Jamaican men in South Florida, aged between 40 and 70 years, and who have undergone PCa screening. The leading interview question will be ‘what participants think about PCa screening sessions, based on their experiences, and whether they are happy that they underwent the procedure’.
Aiken, W. & Eldemire-Shearer, D. (2012). Prostate cancer in Jamaica and the wider Caribbean: It is time to consider screening. West Indian Medical Journal, 61(1), 90-93.
Aiken, W., Tulloch, T., Freeman, V., Bennett. F., Coard, K., Panton, B., &Flanigan, R. (2003).Differences in patient characteristics in Black men with prostate cancer from Jamaica and Chicago. American Society of Clinical Oncology, 22(1), 1764.
Ajzen, I. (1991). The theory of planned behavior. Organizational Behavior and Human Decision Processes, 50(2), 179-211.
American Cancer Society. (2008). Global Cancer: Facts & figures. New York: American Cancer Society, 1-58. Retrieved from http://www.cancer.org/acs/groups/content/@nho/documents/document/2008cafffinalsecuredpdf.pdf
American Cancer Society. (2015). Prostate cancer: What are the risk factors for prostate? Retrieved from http:/www.cancer.org/cancer/prostatecancer/detailedguide/prostate-Cancer-risk-factors
Anderson, B., & Marshall-Lucette, S. (2013). African and Afro-Caribbean men’s experiences of prostate cancer. British Journal of Nursing, 8(22), 1296-1298, 1300-1302, 1304-1307.
Basch, E., Oliver, T. K., Vickers, A., Thompson, I., Kantoff, P., Parnes, H., &Nam, R. K. (2012). Screening for prostate cancer with prostate-specific antigen testing: American Society of Clinical Oncology provisional clinical opinion. Journal of Clinical Oncology, 30(24), 3020-30205. doi: 10.1200/JCO.2012.43.3441
BBC (2015). Jamaica country profile. Available at http://news.bbc.co.uk/2/hi/americas/country_profiles/1190968.stm
Berg, B. (2007). Qualitative Research Methods for the Social Sciences. Boston: Pearson Education.
Berner, E., S. (2009). Diagnostic error in medicine: Introduction. Advances in Health Sciences Education: Theory and Practice, 14(1), 1-5.
Blaikie, N. (2004). Interpretivism. In M. S. Lewis-Beck, A. Bryman, & T. F. Liao (Eds.). Encyclopedia of social science research methods (pp. 509-511).Thousand Oaks, CA: Sage.
Blatter, J. & Blume, T. (2008). In search of co-variance, causal mechanisms or congruence? Towards a plural understanding of case studies. Swiss Political Science Review, 14(2), 315–56
Bowen, D., Hannon, P., Harris. J.,& Martin, D. (2011). Prostate cancer screening and informed decision-making: Provider and patient perspectives. Prostate Cancer and Prostatic Diseases, 14(1), 155-161.
Center, M. M., Jemal, A., Lortet-Tieulent, J., Ward, E., Ferlay, J., Brawley, O., & Bray, F. (2012). International variation in prostate cancer incidence and mortality rates. European Urology. 2012 61 (6), 1079-1092. DOI: 10.1016/j.eururo.2012.02.054.
Centers for Disease Control and Prevention. (2015). Prostate cancer rates by race and ethnicity. Retrieved from http://www.cdc.gov/cancer/prostate/statistics/race.htm
Chan, Z. C., Fung, Y. & Chien, W. (2013). Bracketing in Phenomenology: Only Undertaken in the Data Collection and Analysis Process? The Qualitative Report, 18(59), 1-9
Clarke, T., Soler-Vila, H., Fleming, L, Christ, S., Lee, D., & Arheart, K. (2012). Trends in adherence to recommended cancer screening: The U.S. population and working cancer survivors. Frontiers in Oncology, 2(1), 190-203.
Cohen, L., Manion, L. & Morrison, K.(2007). Research methods in education. New York: Routledge.
Concato, J., Wells, C. K., Horwitz, R. I., Penson, D., Fincke, G., Berlowitz, D. R., & Peduzzi, P. (2006). The effectiveness of screening for prostate cancer: A nested case-control study. Archives of Internal Medicine, 166(1), 38-43.
Consedine, N. S., Adjei, B. A., Horton, D., Joe, A. K., Borrell, L. N., Ramirez, P., & Neugut, A. I. (2009). Fear and loathing in the Caribbean: Three studies of fear and cancer screening in Brooklyn’s immigrant Caribbean subpopulations. Infectious Agents and Cancer, 4(1), 14-18.
Consedine, N. S., Tuck, N. L., Ragin, C. R., & Spencer, B. A. (2015). Beyond the black box: A systematic review of breast, prostate, colorectal, and cervical screening among native and immigrant African-descent Caribbean Populations. Journal of Immigrant Minority Health, 17 (1), 905–924. DOI: 10.1007/s10903-014-9991-0
Creswell, J. W. (2007). Qualitative inquiry and research design: Choosing among five approaches. Thousand Oaks, CA: Sage.
Creswell, J. W., & Miller, D. L. (2000).Determining validity in qualitative inquiry. Theory into Practice, 39(3), 124-130.
Crotty, M. J. (1998). The foundations of social research. London: Sage.
Dang, J., Lee, J., & Tran, J. (2010).Knowledge, attitudes, and beliefs regarding breast and cervical cancer screening among Cambodian, Laotian, Thai, and Tongan Women. Journal of Cancer Education, 25(4), 595-601. doi: 10.1007/s13187-010-0082-1
Djavan, B., Bostanci, Y., & Kazzazi, A. (2015). Chapter 39 Epidemiology, Screening, Pathology and Pathogenesis. In V. H. Nargund, D. Raghavan, & H. M. Sandler (Eds.). Urological Oncology: Incidence and epidemiology (pp. 679 – 681). London: Springer Science/Business Media.
Edelstein, R. S., &Gillath, O. (2008). Avoiding interference: Adult attachment and emotional processing biases. Personality and Social Psychology Bulletin, 34(2), 171-181.
Eldemire-Shearer, D., James, K., Morris, C., Holder-Nevins, D., Lawes, H., & Harris, M. (2011). Chronic disease and ageing in the Caribbean: Opportunities knock at the door. The West Indian Medical Journal, 60(4), 471-477.
Garcia, M., Jemal, A., Ward, E. M., Center, M. M., Hao, Y., Siegel, R. L., & Thun, M. J. (2007). Global cancer facts & figures 2007. American Cancer Society. Retrieved from <https://www.cancer.org/acs/groups/content/@nho/documents/document/globalfactsandfigures2007rev2p.pdf>
Eldemire-Shearer, D., Mitchell-Fearon, K., Laws, H., Waldron, N., James, K., &Holder-Nevins, D. L. (2014). Ageing of Jamaica’s population: What are the implications for healthcare? West Indian Medical Journal, 63(1), 3-8. doi: 10.7727/wimj.2014.003
Ellingson, L. L. (2009). Engaging crystallization in qualitative research: An introduction. Thousand Oaks, CA: Sage
Evans, J., Butler, L., Etowa, J., Crawley, I., Rayson, D., & Bell, D. (2005). Gendered and cultured relations: Exploring African Nova Scotians perceptions and experiences of breast and prostate cancer. Research and Theory for Nursing Practice, 19(1), 257-273.
Finlay, L. (2009). Debating phenomenological research. Phenomenology & Practice, 3(1), 6-25.
Friedman, D., Corwin, S., Rose, I., & Dominick, G. (2009). Prostate cancer communication strategies recommended by older African-American men in South Carolina: A qualitative analysis. Journal of Cancer Education: The Official Journal of the American Association for Cancer Education, 24(3), 204-209.
Garcia, M., Jemal, A., Ward, E. M., Center, M. M., Hao, Y., Siegel, R. L., & Thun, M. J. (2007). Global cancer facts & figures 2007. American Cancer Society. Retrieved fromhttps://www.cancer.org/acs/groups/content/@nho/documents/document/globalfactsandfigures2007rev2p.pdf
Gephart, R. (1999). Paradigms and Research Methods. Academy of Management Research Methods Forum, 4 (1): 1 – 12.
Gibson, T., Hanchard, B., & Waugh, N. (2010).Age-specific incidence of cancer in Kingston and St. Andrew, Jamaica, 2003−2007.West Indian Medical Journal, 59(1), 456-464.
Glennie, A., & Chappell, L. (2010). Jamaica: From Diverse Beginning to Diaspora in the Developed World. Migration Policy Institute. Available at http://www.migrationpolicy.org/article/jamaica-diverse-beginning-diaspora-developed-world
Globocan. (2015). Prostate cancer: Estimated incidence, mortality, and prevalence worldwide in 2012. Report. International Agency for Research on Cancer, World Health Organization. Retrieved from http://globocan.iarc.fr/Pages/fact_sheets_cancer.aspx
Glover, F., Coffey, D. S., Douglas, L. L., Cadogan, M., Russell, H., Tulloch, T., … Walsh, P. C. (1998). The epidemiology of prostate cancer in Jamaica. Journal of Urology, 159(6), 1984-1987.
Grix, J. (2004). The foundations of research. London: Palgrave Macmillan.
Guba, E. G., & Lincoln, Y. S. (1994).Competing paradigms in qualitative research. In N. K. Denzin & Y. S. Lincoln (Eds.), The Sage handbook of qualitative research (pp. 105-117). Thousand Oaks, CA: Sage.
Haas, G., Delongchamps, N., Brawley, O., Wang, C. & De la Roza, G. (2009). The Worldwide Epidemiology of Prostate Cancer: Perspectives from Autopsy Studies. The Canadian Journal of Urology, 15(1), 3866-3871.
Heron, J. & Reason, P. (1997). A participatory enquiry paradigm. Qualitative Inquiry, 3(3), 274-294.
Howrey, B. T., Kuo, Y., Lin, Y., & Goodwin, J. S., (2013). The impact of PSA screening on prostate cancer mortality and over-diagnosis of prostate cancer in the United States. Journal of Gerontology, 68(1), 56-61. doi: 10.1093/gerona/gls135
Husserl, E. (1982). Ideas Pertaining to a Pure Phenomenology and to a Phenomenological Philosophy: First Book, General Introduction to a Pure Phenomenology. (F. Kersten, Trans.). Boston: Kluwer Academic Publishers.
Jeanfreau, S. G., & Jack, L. (2010). Appraising Qualitative Research in Health Education: Guidelines for Public Health Educators. Health Promotion and Practice, 11 (5), 612–617. DOI: 10.1177/1524839910363537.
Jemal, A., Bray, F., Center, M. M., Ferlay, J., Ward, E., & Forman, D. (2011). Global cancer statistics. CA: A Cancer Journal for Clinicians, 61(1), 69-90. doi:10.3322/caac.20107.
Jemal, A., Center, M., DeSantis, C., & Ward, E. M. (2010). Global patterns of cancer incidence and mortality rates and trends. Cancer Epidemiology, Biomarkers & Prevention, 19(1), 1893-1907.
Jones, T. (2008). Jamaican Immigrants in the United States and Canada: Race, Trans-nationalism, and Social Capital. New York, NY: LFB Scholarly Publishing LLC.
Kaplan, B. & Maxwell, J. A. (1994). Qualitative research methods for evaluating computer information systems. In J. G. Anderson C. E. Aydin, & S. J. Jay (Eds.), Evaluating health care information systems, methods and applications (pp. 45-68). Beverly Hills, California: Sage Publications.
Kelliher, F. (2005).Interpretivism and the pursuit of research legitimisation: An integrated approach to single case design.The Electronic Journal of Business Research Methodology, 3(2), 123-132.
Kelly, S., Melnyk, B. M., Jacobson, D. L., &O’Haver, J. A. (2011). Correlates among healthy lifestyle cognitive beliefs, healthy lifestyle choices, social support, and healthy behaviors in adolescents: Implications for behavioral change strategies and future research. Journal of Pediatric Health Care, 25(4), 216-223. DOI:10.1016/j.pedhc.2010.03.002
Kendrick, R. (2010). Erectile dysfunction: A barrier to prostate cancer screening among African American men (Unpublished doctoral dissertation).Capella University. Minneapolis, MN. Retrieved from ProQuest Dissertations & Theses – Gradworks.
Kilpelainen, T. P., Tammela, T. L. J., Maattanen, L., Kujala, P., Stenman, U. H., Ala-Opas, M., &Auvinen, A. (2010). False-positive screening results in the Finnish Prostate Cancer Screening Trial. British Journal of Cancer, 102(1), 469-474. DOI:10.1038/sj.bjc.6605512
Leininger, M. (1969).Ethno-science: A promising research approach to improve nursing practice. Image: Journal of Nursing Scholarship, 3(1), 22-28.
Leininger, M. (2002a). The future of transcultural nursing: A global perspective. In M. Leininger, & M. McFarland (Eds.), Transcultural nursing: Concepts, theories, research, and practice (pp. 577 – 595). New York: McGraw-Hill Medical Publishing Division.
Leininger, M. (2002b). Transcultural nursing and globalization of health care: Importance, focus, and historical aspects. In M. Leininger& M. McFarland (Eds.), Transcultural nursing: Concepts, theories, research, and practice (pp. 3-43). New York: McGraw-Hill Medical Publishing Division.
Leitch, C. M., Hill, F. M., &Harrison, R. T. (2010).The philosophy and practice of interpretivist research in entrepreneurship: Quality, validation, and trust. Organizational Research Methods, 13(1), 67-84.
Lester, S. (1999). An introduction to phenomenological research. Taunton UK, Stan Lester Developments. Retrieved from http://www.academia.edu/1936094/An_introduction_to_phenomenological_research
Lincoln, Y. S., & Guba, E. G. (2013).The constructivist credo. Walnut Creek, CA: Left Coast Press.
Maattanen, L., Hakama, M., Tammela, T. L., Ruutu, M., Ala-Opas, M., Juusela, H., &Auvinen, A. (2007).Specificity of serum prostate-specific antigen determination in the Finnish Prostate Cancer Screening Trial: Randomized controlled trial. British Journal of Cancer, 96(1), 56-60.
Magnus, M (2004). Prostate cancer knowledge among multiethnic Black men. Journal of the National Medical Association, 96(5), 650-656.
Marshall, C. & Rossman, G. B. (2006). Designing qualitative research. Thousand Oaks, California: Sage.
McCree-Hale, R., Hale, T. M., Rutley, K. R., Aung, M., & Jolly, P. E. (2012).Evaluating a theory-based health education intervention to improve awareness of prostate cancer among men in Western Jamaica. West Indian Medical Journal, 61(6), 580-586.
Merriam, S. B. (1998). Qualitative research and case studies applications in education. San Francisco: Jossey-Bass Publications.
Morrison, B., Aiken, W., & Mayhew, R. (2014).Current state of prostate cancer treatment in Jamaica. ECancer Medical Science,8(1), 456-461. doi:10.3332/ecancer.2014.456
Moustakas, C. (1994). Phenomenological research methods. Thousand Oaks, CA: Sage.
Mullally, R. (2003). One Love: The Black Irish of Jamaica. The Jamaica Journal, 42(1), 104–116.
Munhall, P. L. (1994). Revisioning phenomenology: Nursing and health science research. New York, NY: National League of Nursing Press.
Munhall, P. L. (2007). Nursing research: A qualitative perspective. Boston, MA: Jones & Bartlett.
Munhall, P. L. (2012). Nursing research: A qualitative perspective (5th ed.). Sudbury, MA: Jones & Bartlett.
Myers, M. D. (1997). Qualitative research in information systems. MIS Quarterly, 21(2),241 – 242.
Nanton, V., & Dale, J. (2011). It doesn’t make sense to worry too much: The experience of prostate cancer in Afro-Caribbean men in the UK. European Journal of Cancer, 20(1), 62-71.
National Cancer Institute. (2015). SEER Stat Fact Sheets: Prostate Cancer. Surveillance, Epidemiology, and End Results Program, National Cancer Institute. Retrieved fromhttp://seer.cancer.gov/statfacts/html/prost.html
Onyiaorah, I. V., Ukah, C. O., Anyiam, D. C., Onwukamuche, M. E., &Efobi, C. C. (2015). Accuracy of clinical diagnosis of prostate cancer: Implications for patients’ management. Tropical Journal of Medical Research, 18(1), 61-67.
Orlikowski, W. & Baroudi, J. (1991). Studying Information Technology in Organizations: Research Approaches and Assumptions. Information Systems Research, 2 (1): 1 – 28.
Polit, D. F., & Beck, C .T. (2012).Nursing research: Generating and assessing evidence for nursing practice. Philadelphia, PA: Lippincott Williams & Wilkins.
Powers, B. A., & Knapp, T. R. (1995). A dictionary of nursing theory and research. Thousand Oaks, CA: Sage Publications.
Prostate Cancer Caribbean. (2008). Data on prostate cancer in Jamaica. Retrieved fromhttp://pccaribbean.wordpress.com/sitmap/jamaica/data/
Reeves, T., & Hedberg, J. (2003). Interactive Learning Systems Evaluation. Englewood Cliffs, New Jersey: Educational Technology Publications.
Richardson, D., Tibbles, A., & Schwarz, S. (2007). Liverpool and Transatlantic Slavery. London: Liverpool University Press.
Rivera-Ramos, Z. A. &Buki, L. P. (2011). I will no longer be a man! Manliness and prostate cancer screenings among Latino men. Psychology of Men & Masculinity, 12(1), 13-25.
Rodgers, G. (2005). A phenomenological research inquiry of lived experience. Inside Out, 71(1), 19-31.
Ross, L., Dark, T., Orom, H., Underwood, W., Anderson-Lewis, C., Johnson, J., & Erwin, D. (2011).Patterns of information behavior and prostate cancer knowledge among African-American men. Journal of Cancer Education, 26(4), 708–716.
Schwandt, T. (2001). Dictionary of qualitative inquiry. Thousand Oaks, California: Sage.
Sherlock, P., & Bennett, H. (1998). The story of the Jamaican people. New York: Ian Randle Publishers
Sinfield, P., Baker, R., Agarwal, S., & Tarrant, C. (2008). Patient-centered care: What are the experiences of prostate cancer patients and their partners? Patient Education and Counseling, 73,91-96.
Taitt, H. (2015). Prostate cancer and Afro-Caribbean men: Experiences, perceptions, and beliefs (Doctoral dissertation). Walden University, Minneapolis, MN. Dissertations and Doctoral Studies – ScholarlyWorks. Retrieved from <http://scholarworks.waldenu.edu/cgi/viewcontent.cgi?article=1303&context=dissertations
Upadhyay, P. (2012). Interpretivist tradition in qualitative anthropological research writings. Himalayan Journal of Sociology and Anthropology, 5(1), 123-137.
Van Maanen, J. (1988). Tales of the Field. Chicago, IL: Chicago University Press.
van Manen, J.(1990). Researching lived experience: Human science for an action sensitive pedagogy. New York: Albany State University of New York Press.
Willis, J. (1995). Recursive, Reflective Instructional Design Model Based on Constructivist-Interpretist Theory. Educational Technology, 35(6): 5 – 23.
Yin, R. (2003). Case Study Research Design and Methods. New York: Sage Publications.
Appendix A: Sample of Face-to-Face Interview Questions
Sample Schedule for face-To-face Interviews(Jamaican Men Residing in South Florida, Between Ages of 40 – 70 Years) |
Part A: Introduction Brief |
Lived Experience of Jamaican Men after Undergoing Prostate Cancer Screening The purpose of the present research is to: Conduct a phenomenological exploration of lived experience of Jamaican men residing in the US, after undergoing PCa screening.Thank you for accepting to participate in this study, upon referral. You are guaranteed of full confidentiality for your participation. Nothing you say during this interview will be linked to or identified by your name, or personal identity in the documentation of the study The information provide during our interviews shall be treated confidentially, only for the purposes of this study and shall not be provided to any other third party for any purpose whatsoever If there is any question during the interview you do not understand, or any form of clarification you need, please feel free to inform me at any time. |
Part B: Demographic Data |
Please Tell Me a Few Details About Yourself… Name: __________ ________________ ___________Age: __________ yearsNationality of Origin: ________________Country of Residence: ________________Education Level: _______________________________Marital Status: ________________Children: ________________Ever Attended a PC Screening: ___________ and if so, When ________________ |
Part C: Main Body of Research Interests |
Leading Interview Question What do you feel/think about PCa screening sessions, based on your experiences? Are you happy that you underwent the procedure?’ |
Follow Up Questions Why did you attend the PCa screening session?Was it your first session or one among many sessions you have undergone?How old were you when you realized or heard about the need for PCa screening for Jamaican men, or for men in general?So, why did you attend the PCa screening session?Were you surprised about what they had to do to you, during the PCa screening session?Did you know exactly what to expect during the PCa screening session?Did it matter who conducted the PCa screening procedure, in terms of gender and age? How did you feel during and after the PCa screening procedure?What do you think now about the PCa screening procedure?What about the PCa screening procedure was offensive to you, if any?Do you think that attending PCa screening sessions is important for Jamaican men? Why?What about PCa screening would you like done differently, based on your experience?As a Jamaican man, do you feel that other Jamaican men should adherently attend PCa screening sessions now? If there were any other way of testing for PCa, would you prefer the alternative or the screening procedure? Would you like to, and will you, attend another PCa screening session after one or two years?In summary therefore, what do you feel/think about PCa screening sessions, based on your experiences? Are you happy that you underwent the procedure? |
Part D: Survey Summary |
Is there anything else you like to share with me on PCa screening for Jamaican men?—————————————————————————————————————————————————————————————————————————————————————————————————— Thinking about the areas we have covered in this interview, especially in regards to the experiences of Jamaican men during PC screening, is there anything else that you would like to add? If Yes, Please Explain:—————————————————————————————————————————————————————————————————————————————————————————————————— |
That will be all.Thank you for your time and participation in this study. Your contribution is highly appreciated. |
Delivering a high-quality product at a reasonable price is not enough anymore.
That’s why we have developed 5 beneficial guarantees that will make your experience with our service enjoyable, easy, and safe.
You have to be 100% sure of the quality of your product to give a money-back guarantee. This describes us perfectly. Make sure that this guarantee is totally transparent.
Read moreEach paper is composed from scratch, according to your instructions. It is then checked by our plagiarism-detection software. There is no gap where plagiarism could squeeze in.
Read moreThanks to our free revisions, there is no way for you to be unsatisfied. We will work on your paper until you are completely happy with the result.
Read moreYour email is safe, as we store it according to international data protection rules. Your bank details are secure, as we use only reliable payment systems.
Read moreBy sending us your money, you buy the service we provide. Check out our terms and conditions if you prefer business talks to be laid out in official language.
Read more